Department of Nephrology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, China.
Key Laboratory of Nephrology, Ministry of Health and Guangdong Province, Guangzhou, China.
BMC Nephrol. 2018 Oct 26;19(1):297. doi: 10.1186/s12882-018-1092-1.
Inflammation-based prognostic scores have been used as outcome predictors in patients with cancer or on hemodialysis. However, their role in patients on continuous ambulatory peritoneal dialysis (CAPD) remains unclear. This study aimed to examine the prognostic value of inflammation-based composite scores for mortality in CAPD patients.
This study was conducted in CAPD patients enrolled from January 1, 2006 to December 31, 2014 and followed until December 31, 2016. Three inflammation-based prognostic scores, including Glasgow prognostic score (GPS), prognostic nutritional index (PNI), and prognostic index (PI), were conducted in this study. The associations between these scores and all-cause or cardiovascular mortality were evaluated by Kaplan-Meier method and Cox proportional hazards models. The areas under the curve (AUC) of receiver-operating characteristic (ROC) analysis were used to determine the predictive values of mortality.
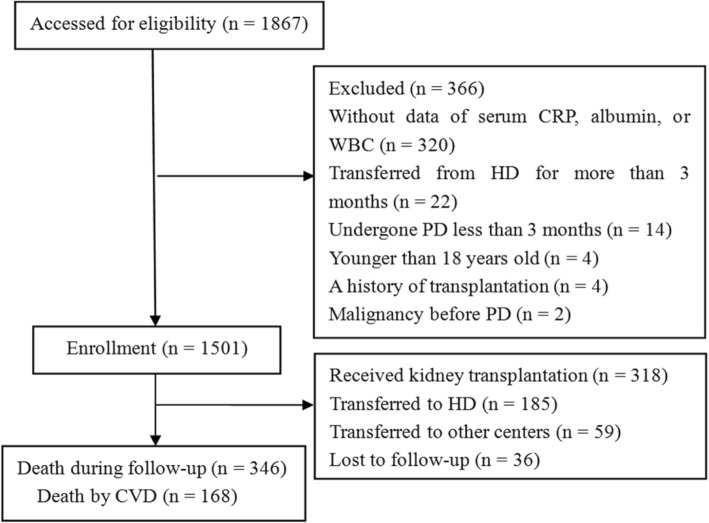
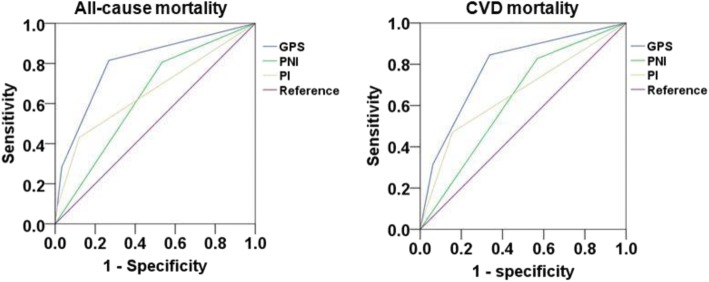
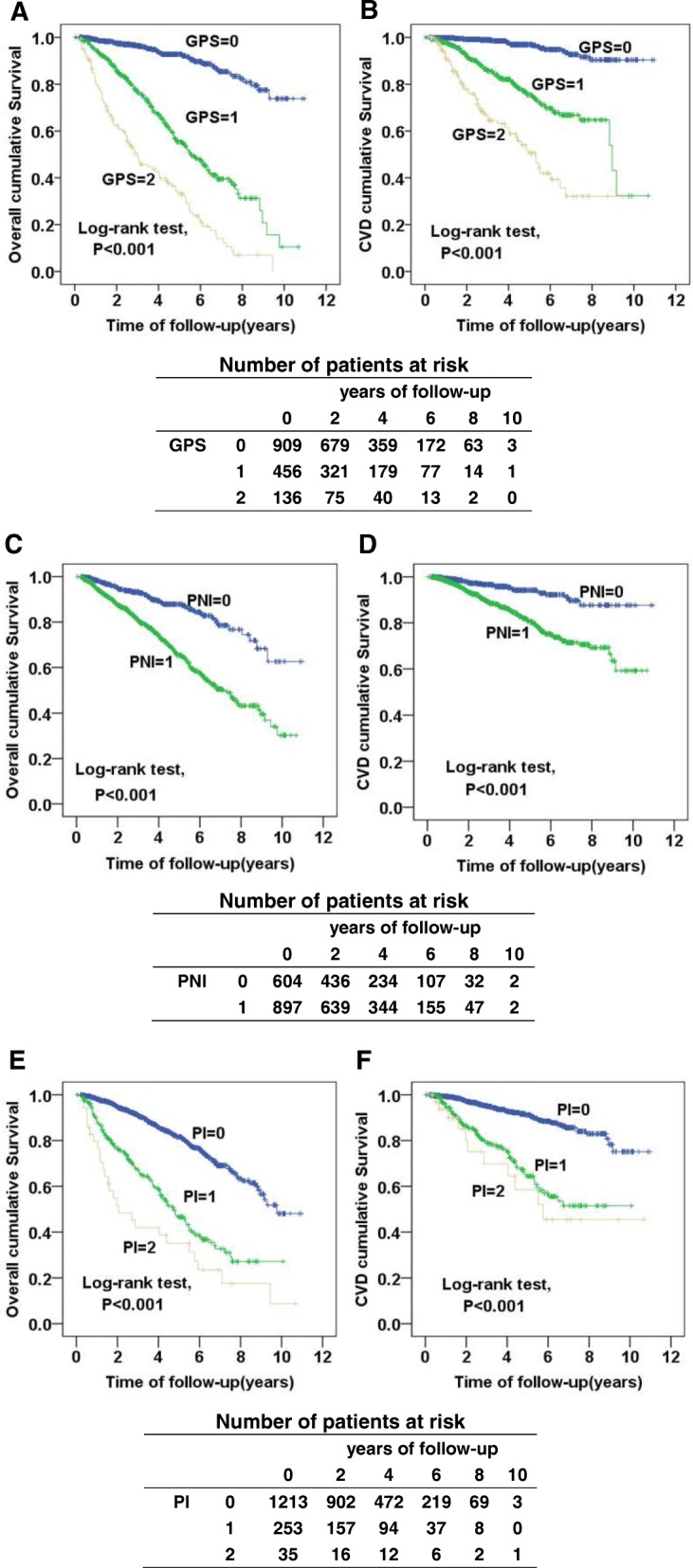
A total of 1501 patients were included. During a median follow-up of 38.7 (range, 21.6-62.3) months, 346 (23.1%) patients died, of which 168 (48.6%) were due to cardiovascular diseases (CVD). After adjustment for confounders, the results showed that elevated GPS, PNI, and PI scores were all independently associated with all-cause [GPS: Score 1: hazard ratio(HR) 3.94, 95% confidence interval(CI) 2.90-5.35; Score 2: HR 7.56, 95% CI 5.35-10.67; PNI: HR 1.82, 95% CI 1.36-2.43; PI: Score 1: HR 2.08, 95% CI 1.63-2.65; Score 2: HR 3.03, 95% CI 2.00-4.60)] and CVD mortality(GPS: Score 1: HR 4.41, 95% CI 2.76-7.03; Score 2: HR 9.64, 95% CI 5.72-16.26; PNI: HR 1.63, 95% CI 1.06-2.51; PI: Score 1: HR 2.57, 95% CI 1.81-3.66, Score 2: HR 3.85, 95% CI 1.99-7.46).The AUC values of GPS score were 0.798 (95% CI0.770-0.826) for all-cause mortality and 0.781 (95% CI 0.744-0.817) for CVD mortality, both of which significantly higher than those of PNI and PI scores (P < 0.001, respectively).
All elevated GPS, PNI, and PI scores were independently associated with all-cause and CVD mortality. The GPS score showed better predictive value than PNI and PI scores in CAPD patients.
炎症相关的预后评分已被用于预测癌症或血液透析患者的结局。然而,其在持续不卧床腹膜透析(CAPD)患者中的作用尚不清楚。本研究旨在探讨炎症相关综合评分对 CAPD 患者死亡率的预后价值。
本研究纳入了 2006 年 1 月 1 日至 2014 年 12 月 31 日期间登记的 CAPD 患者,并随访至 2016 年 12 月 31 日。本研究采用了三种炎症相关的预后评分,包括格拉斯哥预后评分(GPS)、预后营养指数(PNI)和预后指数(PI)。采用 Kaplan-Meier 法和 Cox 比例风险模型评估这些评分与全因或心血管死亡率的关系。通过受试者工作特征(ROC)分析的曲线下面积(AUC)来确定死亡率的预测价值。
共纳入 1501 例患者。中位随访时间为 38.7(范围 21.6-62.3)个月,346(23.1%)例患者死亡,其中 168(48.6%)例死于心血管疾病(CVD)。在调整混杂因素后,结果显示,升高的 GPS、PNI 和 PI 评分均与全因死亡[GPS:评分 1:风险比(HR)3.94,95%置信区间(CI)2.90-5.35;评分 2:HR 7.56,95% CI 5.35-10.67;PNI:HR 1.82,95% CI 1.36-2.43;PI:评分 1:HR 2.08,95% CI 1.63-2.65;评分 2:HR 3.03,95% CI 2.00-4.60]和 CVD 死亡率(GPS:评分 1:HR 4.41,95% CI 2.76-7.03;评分 2:HR 9.64,95% CI 5.72-16.26;PNI:HR 1.63,95% CI 1.06-2.51;PI:评分 1:HR 2.57,95% CI 1.81-3.66,评分 2:HR 3.85,95% CI 1.99-7.46)]相关。GPS 评分的 AUC 值为 0.798(95%CI0.770-0.826)用于全因死亡率,0.781(95%CI 0.744-0.817)用于 CVD 死亡率,均显著高于 PNI 和 PI 评分(P < 0.001)。
所有升高的 GPS、PNI 和 PI 评分均与全因和 CVD 死亡率独立相关。GPS 评分在 CAPD 患者中的预测价值优于 PNI 和 PI 评分。