1 Aston Medical Research Institute Aston Medical School Aston University Birmingham United Kingdom.
2 Centre for Cardiovascular Sciences University of Birmingham United Kingdom.
J Am Heart Assoc. 2018 Aug 21;7(16):e008508. doi: 10.1161/JAHA.117.008508.
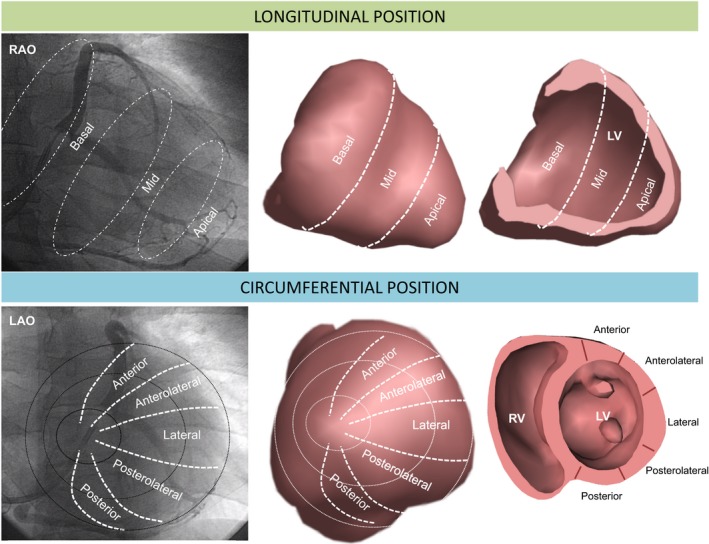
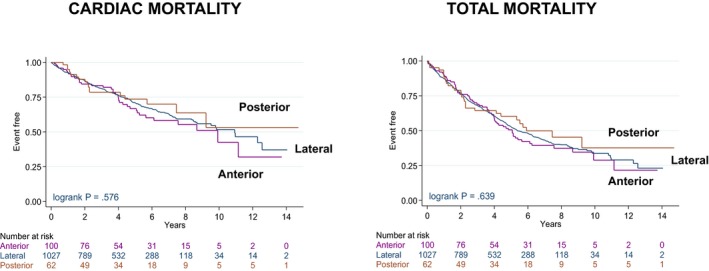
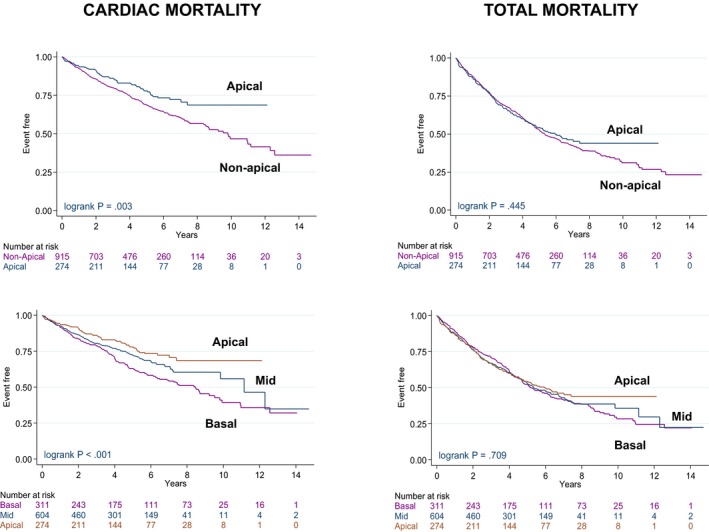
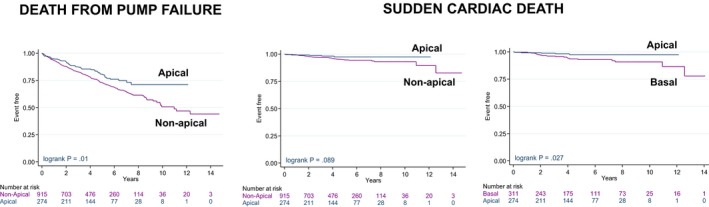
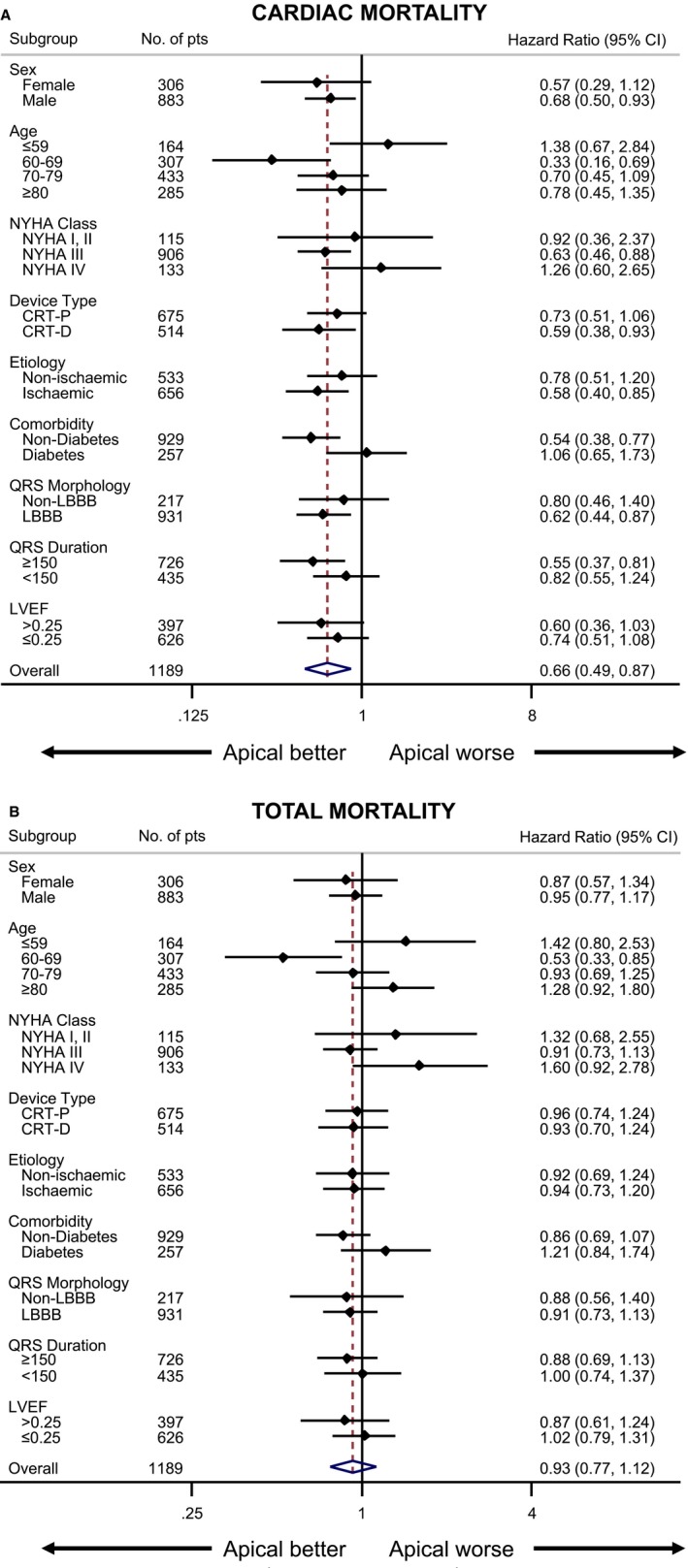
Background Experimental evidence indicates that left ventricular ( LV ) apical pacing is hemodynamically superior to nonapical LV pacing. Some studies have shown that an LV apical lead position is unfavorable in cardiac resynchronization therapy. We sought to determine whether an apical LV lead position influences cardiac mortality after cardiac resynchronization therapy. Methods and Results In this retrospective observational study, the primary end point of cardiac mortality was assessed in relation to longitudinal (basal, midventricular, or apical) and circumferential (anterior, lateral, or posterior) LV lead positions, as well as right ventricular (apical or septal), assigned using fluoroscopy. Lead positions were assessed in 1189 patients undergoing cardiac resynchronization therapy implantation over 15 years. After a median follow-up of 6.0 years (interquartile range: 4.4-7.7 years), an apical LV lead position was associated with lower cardiac mortality than a nonapical position (adjusted hazard ratio: 0.74; 95% confidence interval, 0.56-0.99) after covariate adjustment. There were no differences in total mortality or heart failure hospitalization. Death from pump failure was lower with apical than nonapical positions (adjusted hazard ratio: 0.69; 95% confidence interval, 0.51-0.94). Compared with a basal position, an apical LV position was also associated with lower risk of sudden cardiac death (adjusted hazard ratio: 0.34; 95% confidence interval, 0.13-0.93). No differences emerged between circumferential LV lead positions or right ventricular positions with respect to any end point. Conclusions In recipients of cardiac resynchronization therapy, an apical LV lead position was associated with better long-term cardiac survival than a nonapical position. This effect was due to a lower risk of pump failure and sudden cardiac death.
实验证据表明,左心室(LV)心尖部起搏在血流动力学方面优于非心尖部 LV 起搏。一些研究表明,LV 心尖部导联位置不利于心脏再同步治疗。我们旨在确定心脏再同步治疗后 LV 心尖部导联位置是否影响心脏死亡率。
在这项回顾性观察性研究中,我们评估了心脏死亡率与 LV 心尖部(基底、中室或心尖部)和圆周(前、侧或后)导联位置之间的关系,以及右心室(心尖部或间隔部)的关系,这些位置是使用透视术分配的。在 1189 名接受心脏再同步治疗植入术的患者中评估了导联位置。在中位随访 6.0 年(四分位间距:4.4-7.7 年)后,在调整了协变量后,与非心尖部位置相比,LV 心尖部导联位置与较低的心脏死亡率相关(调整后的危险比:0.74;95%置信区间:0.56-0.99)。总死亡率或心力衰竭住院率无差异。心尖部位置的泵衰竭死亡率低于非心尖部位置(调整后的危险比:0.69;95%置信区间:0.51-0.94)。与基底位置相比,LV 心尖部位置与较低的心脏性猝死风险相关(调整后的危险比:0.34;95%置信区间:0.13-0.93)。在圆周 LV 导联位置或右心室位置方面,任何终点均无差异。
在接受心脏再同步治疗的患者中,LV 心尖部导联位置与非心尖部位置相比,长期心脏生存率更好。这种效果归因于泵衰竭和心脏性猝死风险降低。