Li Jianbo, Wang Chengdi, Jiang Yuting, Song Jiulin, Zhang Longhao, Chen Nan, Zhang Rui, Yang Lan, Yao Qin, Jiang Li, Yang Jian, Zhu Tao, Yang Yang, Li Weimin, Yan Lunan, Yang Jiayin
Department of Liver Surgery and State Key Laboratory of Biotherapy, West China Hospital.
Department of Respiratory and Critical Care Medicine, West China Medical School/West China Hospital.
Medicine (Baltimore). 2018 Nov;97(45):e13082. doi: 10.1097/MD.0000000000013082.
To systematically compare immediate postoperative tracheal extubation (IPTE) with conventional tracheal extubation (CTE) and to determine whether IPTE can achieve an enhanced recovery for adult patients underwent liver transplantation (LT) without additional risks. We designed a systematic review and meta-analysis.
The RCTs, cohorts, case-controls, or case series that explored outcomes of IPTE after LT for adults were involved in our study. The Newcastle-Ottawa scale was used to assess the risk of bias.
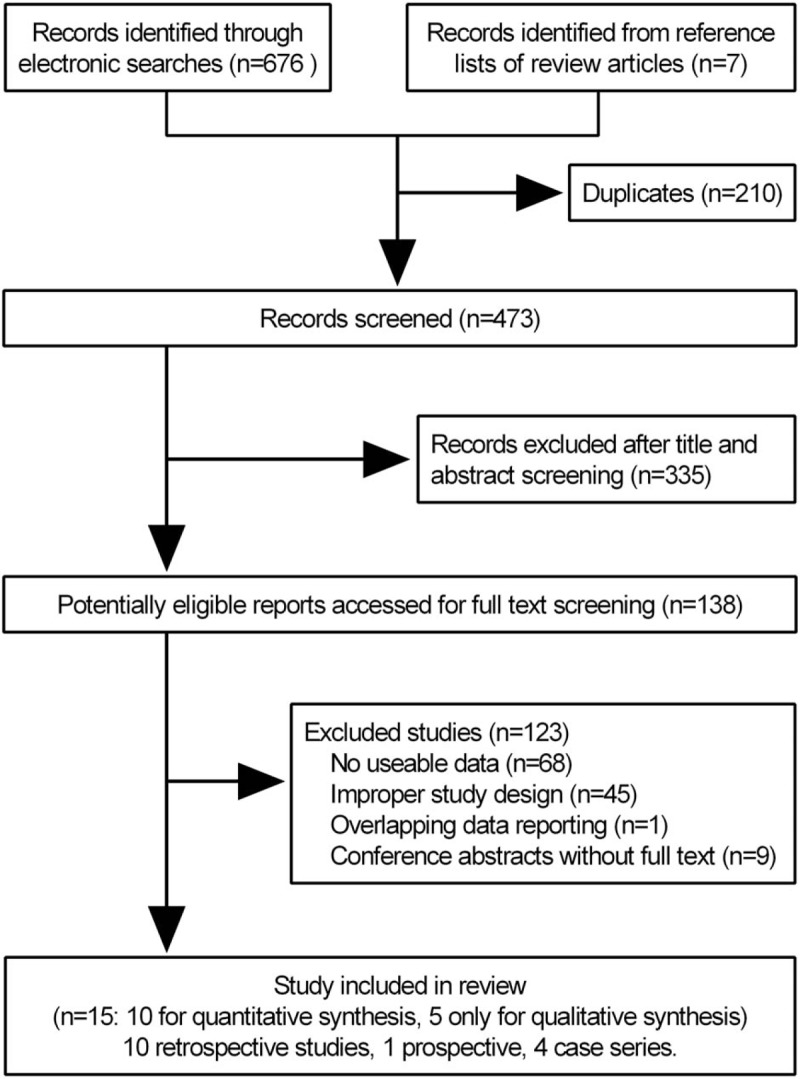
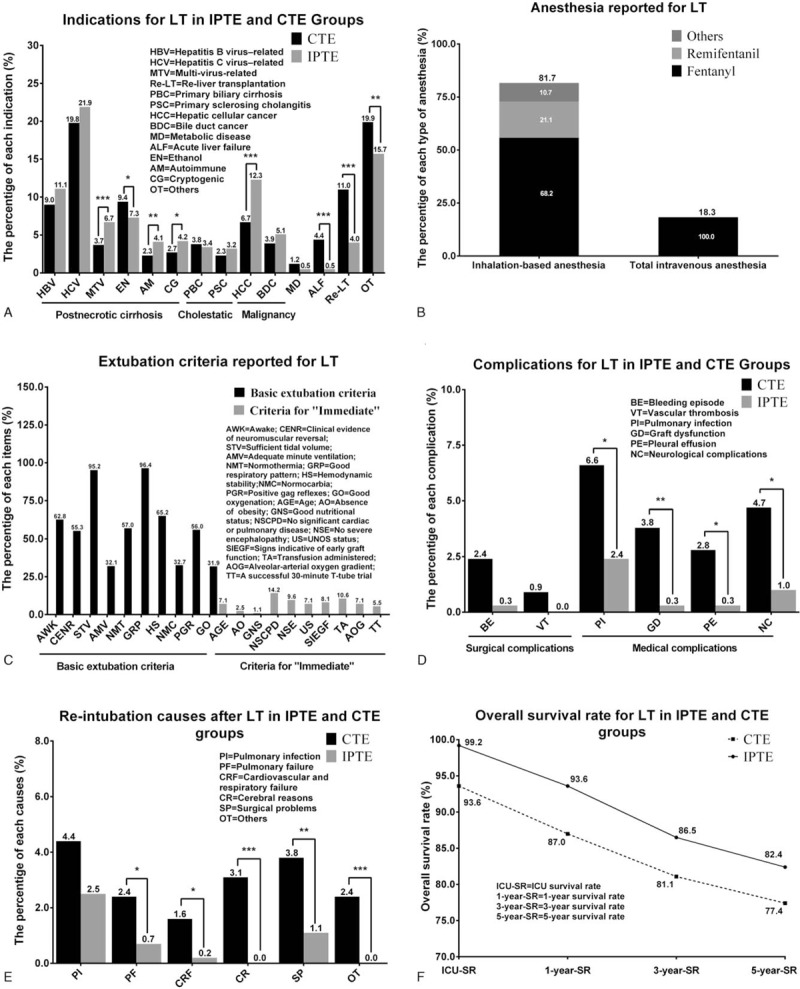
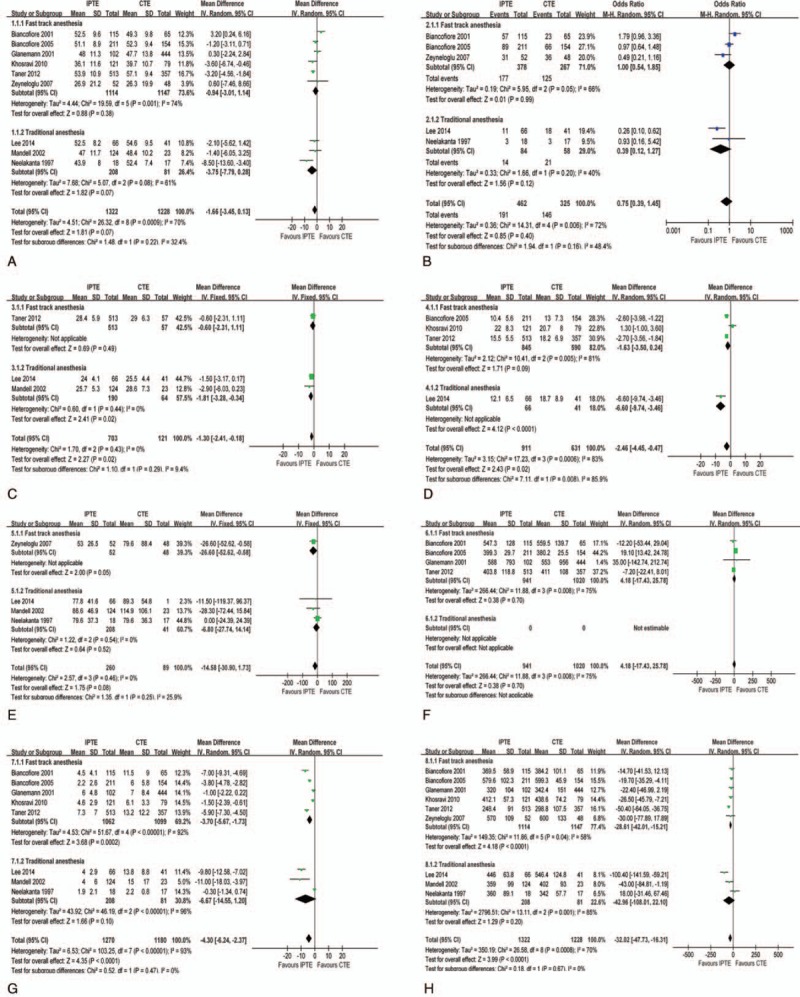
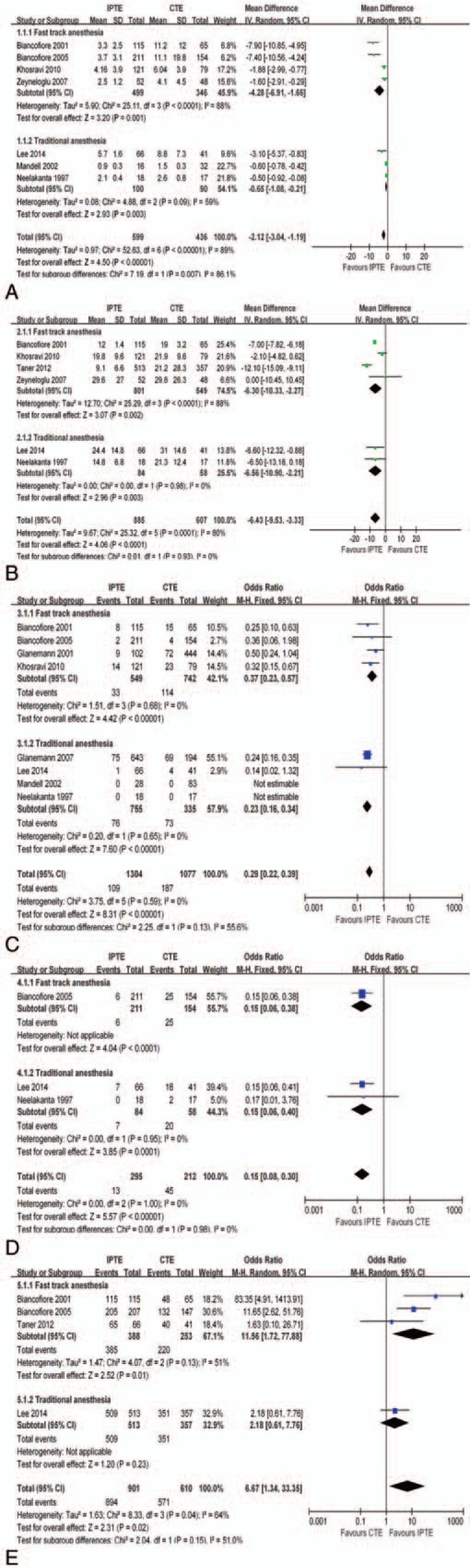
A total of 15 studies (n = 4144) were included, consisting of 10 studies (retrospective cohorts; n = 3387) for quantitative synthesis and 5 studies (1 prospective cohort, and 4 case series; n = 757) for qualitative synthesis. The pooled estimates suggested IPTE could reduce time to discharge from ICU stay (TDICU) (mean difference [MD] -2.12 days, 95% confidence interval [CI] -3.04 to -1.19 days), time to discharge from the hospital (TDH) (MD -6.43 days, 95% CI -9.53 to -3.33 days), re-intubation rate (RI) (odds ratio [OR] 0.29, 95% CI 0.22-0.39), morbidity rate (MR) (OR 0.15, 95% CI 0.08-0.30) and graft dysfunction rate (GD) (IPTE vs CTE: 0.3% vs 3.8%, P < .01), and had comparable ICU survival rate (ICUS) (OR 6.67 95% CI 1.34-33.35) when compared with CTE after LT.
IPTE can achieve an enhanced recovery for adult patients underwent LT without additional re-intubation, morbidity, and mortality risks. However, further work needs to be done to establish the extent definitively through carefully designed and conducted RCTs.
系统比较成人肝移植(LT)术后即刻气管拔管(IPTE)与传统气管拔管(CTE),并确定IPTE是否能在不增加额外风险的情况下实现成人肝移植患者的加速康复。我们设计了一项系统评价和荟萃分析。
纳入探索成人LT术后IPTE结局的随机对照试验(RCT)、队列研究、病例对照研究或病例系列。采用纽卡斯尔-渥太华量表评估偏倚风险。
共纳入15项研究(n = 4144),其中10项研究(回顾性队列研究;n = 3387)用于定量合成,5项研究(1项前瞻性队列研究和4项病例系列研究;n = 757)用于定性合成。汇总估计表明,与LT术后CTE相比,IPTE可缩短重症监护病房(ICU)住院时间(MD -2.12天,95%置信区间[CI] -3.04至-1.19天)、住院时间(MD -6.43天,95% CI -9.53至-3.33天)、再插管率(RI)(比值比[OR] 0.29,95% CI 0.22 - 0.39)、发病率(MR)(OR 0.15,95% CI 0.08 - 0.30)和移植物功能障碍率(GD)(IPTE与CTE:0.3%对3.8%,P < 0.01),且ICU生存率(ICUS)相当(OR 6.67,95% CI 1.34 - 33.35)。
IPTE可在不增加额外再插管、发病率和死亡率风险的情况下实现成人LT患者的加速康复。然而,需要通过精心设计和实施的RCT进一步明确其确切程度。