Université de Sherbrooke, 580 Rue Bowen S, Sherbrooke, QC, J1G 2E8, Canada.
University of Alberta, Room 1E4, W.C.M. Health Sciences Centre, 8440-112 Street, Edmonton, AB, T6G 2B7, Canada.
J Otolaryngol Head Neck Surg. 2018 Nov 8;47(1):67. doi: 10.1186/s40463-018-0313-8.
Chronic rhinosinusitis (CRS) affects up to 16% of the population. When medical treatment fails, endoscopic sinus surgery (ESS) is considered. The value of resecting the middle turbinate to optimize surgical outcomes has been hypothesized but remains controversial and unproven. Whether the middle turbinate should be left in place or resected is controversial. Our objective is to determine if middle turbinectomy improves objective surgical outcomes after ESS.
Sixteen patients (15 men, 15 primary surgery) undergoing bilateral complete ESS for CRS with nasal polyposis were recruited. Nasal cavities were randomized so that middle turbinectomy was performed on one side while the middle turbinate was preserved on the other. Each participant acted as their own control. Nasal cavities were compared using Perioperative Sinus Endoscopy (POSE) and Lund-Kennedy (LKES) scores pre-operatively, and at 1, 3 and 6 months after ESS. Results were analyzed using Wilcoxon signed-rank test.
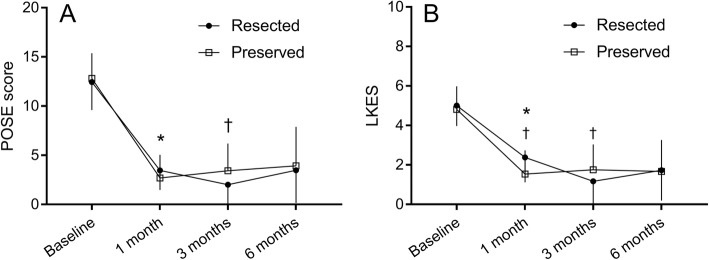
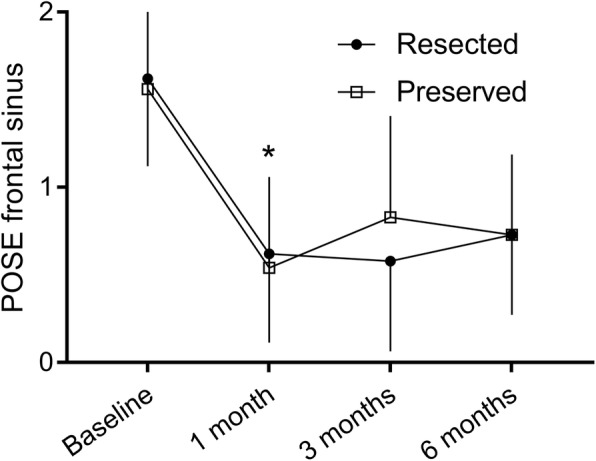
Pre-operatively, the POSE (12.4 ± 2.9 vs 12.8 ± 2.6, p = 0.33, for the preserved side and the resected side, respectively) and LKES (5.0 ± 1.0 vs 4.8 ± 1.2, p = 0.33) scores were similar between sides. During follow up, resection was associated with more crusting at 1 month following ESS (1.0 ± 0.7 vs 0.4 ± 0.6, p = 0.02). There was a small, but statistically significant, difference between the nasal cavities at 3 months, where the resected side showed better endoscopic appearance (2.0 ± 2.2 vs 3.4 ± 2.8, p = 0.01). No difference was found at 6 months. Frontal sinus scores were similar between sides at 6 months (0.7 ± 0.5 vs 0.7 ± 0.5, p = 1.00).
Our results show no sustained objective endoscopic benefit of routine middle turbinectomy, at least within the first six postoperative months, in patients undergoing primary ESS for CRS with polyposis.
NCT, NCT02855931 . Registered 16 August 2016.
慢性鼻-鼻窦炎(CRS)影响了高达 16%的人群。当医学治疗失败时,内镜鼻窦手术(ESS)被认为是一种治疗方法。切除中鼻甲以优化手术结果的价值已被假设,但仍存在争议,且尚未得到证实。中鼻甲是否应保留或切除仍存在争议。我们的目的是确定中鼻甲切除术是否能改善 ESS 后的客观手术结果。
招募了 16 名(15 名男性,15 名初次手术)患有鼻息肉的 CRS 患者,他们接受了双侧完整的 ESS。鼻腔随机分组,一侧行中鼻甲切除术,另一侧保留中鼻甲。每个参与者都作为自己的对照。术前、术后 1、3 和 6 个月使用围手术期鼻窦内镜(POSE)和 Lund-Kennedy(LKES)评分比较鼻腔。结果采用 Wilcoxon 符号秩检验进行分析。
术前,保留侧和切除侧的 POSE(12.4±2.9 与 12.8±2.6,p=0.33)和 LKES(5.0±1.0 与 4.8±1.2,p=0.33)评分相似。在随访期间,ESS 后 1 个月,切除侧的结痂更多(1.0±0.7 与 0.4±0.6,p=0.02)。3 个月时,切除侧的内镜表现稍好,但差异具有统计学意义(2.0±2.2 与 3.4±2.8,p=0.01)。6 个月时无差异。6 个月时,额窦评分在两侧相似(0.7±0.5 与 0.7±0.5,p=1.00)。
我们的结果显示,在接受初次 ESS 治疗伴有息肉的 CRS 的患者中,常规中鼻甲切除术至少在术后 6 个月内并没有持续的客观内镜获益。
NCT02855931。2016 年 8 月 16 日注册。