Structural Heart and Valve Center, Vanderbilt University School of Medicine, Nashville, Tennessee.
Quebec Heart and Lung Institute, Quebec City, Canada.
JACC Cardiovasc Interv. 2018 Nov 12;11(21):2172-2181. doi: 10.1016/j.jcin.2018.07.039.
This study sought to evaluate whether a multimarker approach might identify patients with higher mortality and hospitalization rates after aortic valve replacement (AVR) for aortic stenosis (AS).
The society valve guidelines include accepted triggers for AVR in patients with severe asymptomatic AS, but circulating biomarkers do not have a clear role.
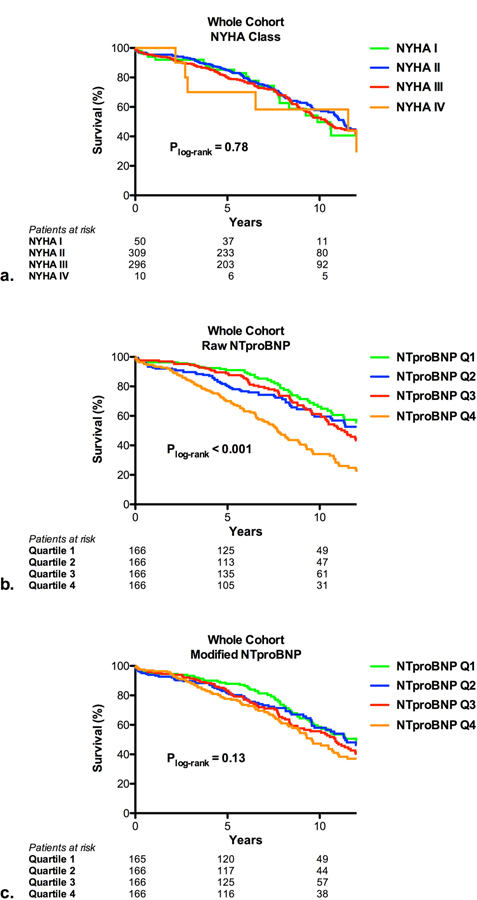
From a prospective registry of patients undergoing cardiac surgery between 2000 and 2012, 665 treated with surgical AVR (441 isolated) were evaluated. Seven biomarkers were measured on blood samples obtained before AVR. Biomarker levels were adjusted to account for the influence of age, sex, body mass index, and renal function; the median was used to determine an elevated value. Endpoints included all-cause mortality and all-cause and cardiovascular hospitalizations. Mean follow-up was 10.7 years and 299 (45%) died.
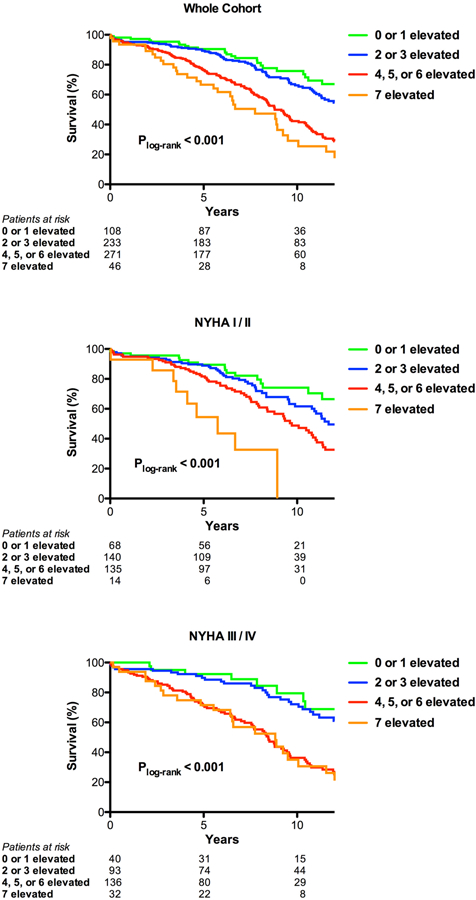
Patients with 0 to 1, 2 to 3, 4 to 6, and 7 biomarkers elevated had 5-year mortality of 10%, 12%, 24%, and 33%, respectively, and 10-year mortality of 24%, 35%, 58%, and 71%, respectively (log-rank p < 0.001). The association between an increasing number of elevated biomarkers and increased all-cause mortality was observed among those with minimal symptoms (New York Heart Association functional class I or II) and those with a low N-terminal pro-B-type natriuretic peptide (p < 0.01 for both). Compared with those with 0 to 1 biomarkers elevated, patients with 4 to 6 or 7 biomarkers elevated had an increased hazard of mortality after adjustment for clinical risk scores (p < 0.01) and a 2- to 3-fold higher rate of all-cause and cardiovascular rehospitalization after AVR. Similar findings were obtained when evaluating cardiovascular mortality. Among patients with no or minimal symptoms, 42% had ≥4 biomarkers elevated.
Among patients with severe AS treated with surgical AVR, an increasing number of elevated biomarkers of cardiovascular stress was associated with higher all-cause and cardiovascular mortality and a higher rate of repeat hospitalization. A multimarker approach may be useful in the surveillance of asymptomatic patients with severe AS to optimize surgical timing.
本研究旨在评估多标志物方法是否可用于识别主动脉瓣置换术(AVR)治疗主动脉瓣狭窄(AS)后死亡率和住院率较高的患者。
社会瓣膜指南包含了严重无症状 AS 患者接受 AVR 的公认触发因素,但循环生物标志物在这方面没有明确的作用。
从 2000 年至 2012 年接受心脏手术的前瞻性患者注册中,评估了 665 例接受手术 AVR(441 例单纯性)的患者。在 AVR 前采集血液样本,测量 7 种生物标志物。对生物标志物水平进行调整,以考虑年龄、性别、体重指数和肾功能的影响;使用中位数来确定升高的值。终点包括全因死亡率和全因及心血管住院率。平均随访 10.7 年,299 例(45%)死亡。
生物标志物升高 0 至 1、2 至 3、4 至 6 和 7 个标志物的患者,5 年死亡率分别为 10%、12%、24%和 33%,10 年死亡率分别为 24%、35%、58%和 71%(对数秩检验 p<0.001)。在有轻微症状(纽约心脏协会功能分级 I 或 II)和低 N 末端前 B 型利钠肽(p<0.01)的患者中,观察到生物标志物升高数量与全因死亡率增加之间存在关联。与生物标志物升高 0 至 1 个标志物的患者相比,生物标志物升高 4 至 6 个或 7 个标志物的患者,在校正临床风险评分后,死亡风险增加(p<0.01),AVR 后全因和心血管再住院率增加 2 至 3 倍。当评估心血管死亡率时,也得到了类似的结果。在无症状或症状轻微的患者中,42%的患者有≥4 个标志物升高。
在接受手术 AVR 治疗的严重 AS 患者中,心血管应激的生物标志物升高数量增加与全因和心血管死亡率增加以及再住院率增加相关。多标志物方法可能有助于无症状严重 AS 患者的监测,以优化手术时机。