Department of Orthopaedic Surgery, Medical University of Vienna, Waehringer Guertel 18-20, 1090, Vienna, Austria.
Center for Medical Statistics, Informatics, and Intelligent Systems - Section for Clinical Biometrics, Medical University of Vienna, Waehringer Guertel 18-20, 1090, Vienna, Austria.
Sci Rep. 2018 Nov 8;8(1):16148. doi: 10.1038/s41598-018-34397-5.
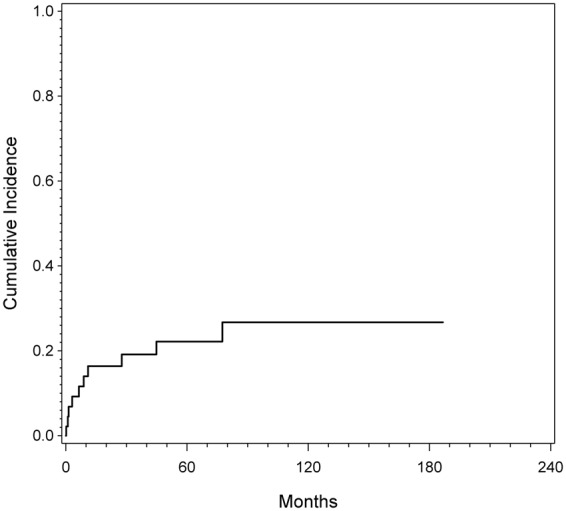
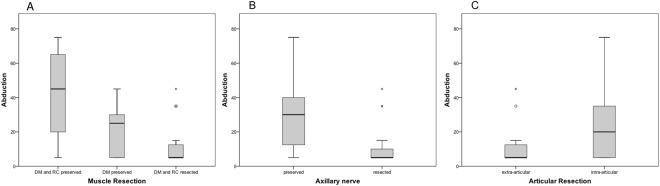
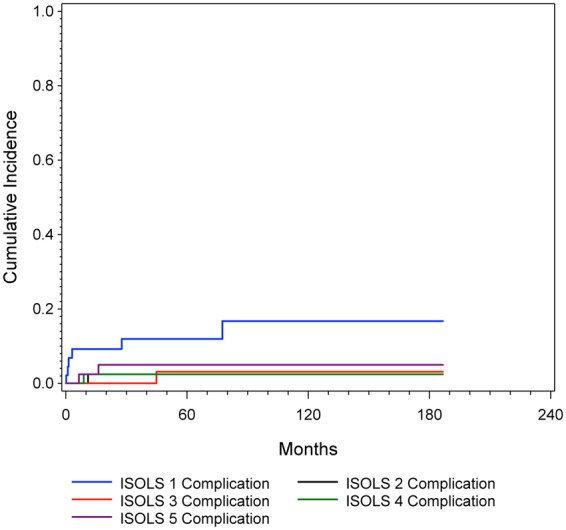
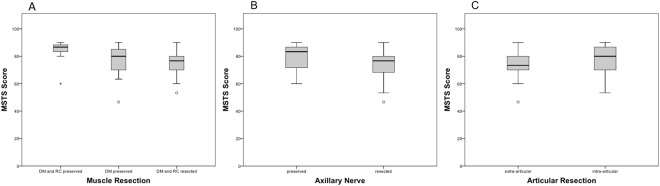
Endoprosthetic reconstruction (EPR) is the most widely used reconstruction technique after humeral osteosarcoma (OSA). Complications are common and function is often compromised due to the premise of wide resection. In the current study we evaluated (1) the risk of complications after resection and EPR; (2) the functional outcome and how it is influenced by the preservation/resection of deltoid muscle (DM), rotator cuff (RC), axillary nerve or the type of resection (intra-/extraarticular) and (3) if the preservation/resection of DM, RC, axillary nerve or the type of resection has a negative influence on the oncological outcome. We retrospectively evaluated data of 49 patients with humeral OSA. All patients underwent resection and EPR. Complication-free survival according to the ISOLS classification was estimated by a competing risk model. Functional outcome was evaluated by range of motion (ROM) in abduction and the MSTS score. Eleven patients (22%) had at least one complication. The estimated cumulative incidence for the first complication was 18% at one year, 23% at five years, and 28% at ten years, respectively. Soft tissue failure was the most common complication. ROM and MSTS scores were significantly higher in patients where DM and RC (p = 0.043/p = 0.046) and axillary nerve (p = 0.014/p = 0.021) could be preserved. Preservation of these structures had no negative influence on the surgical margins. In conclusion, EPR is a good treatment method with an acceptable complication rate. Preservation of the abductor mechanism, when possible in the setting of obtaining negative margins, provides superior functional outcome.
人工假体重建(EPR)是肱骨骨肉瘤(OSA)后最广泛使用的重建技术。由于广泛切除的前提,并发症很常见,功能往往受到影响。在本研究中,我们评估了:(1)切除和 EPR 后的并发症风险;(2)功能结果以及三角肌(DM)、肩袖(RC)、腋神经的保留/切除、关节内/外切除的类型如何影响功能结果;(3)DM、RC、腋神经的保留/切除或切除类型是否对肿瘤学结果有负面影响。我们回顾性评估了 49 例肱骨骨肉瘤患者的数据。所有患者均行切除术和 EPR。采用竞争风险模型估计根据 ISOLS 分类的无并发症生存情况。通过外展范围的运动范围(ROM)和 MSTS 评分评估功能结果。11 例(22%)至少有 1 例并发症。第 1 次并发症的估计累积发生率分别为 1 年时 18%,5 年时 23%,10 年时 28%。软组织失败是最常见的并发症。DM 和 RC(p=0.043/p=0.046)和腋神经(p=0.014/p=0.021)可保留的患者的 ROM 和 MSTS 评分明显更高。保留这些结构对手术切缘无负面影响。总之,EPR 是一种具有可接受并发症发生率的良好治疗方法。在获得阴性切缘的前提下,尽可能保留外展肌机制可提供更好的功能结果。