Division of Hematology, Department of Internal Medicine, Mayo Clinic, Rochester, MN.
Center of Research and Innovation of Myeloproliferative Neoplasms, University of Florence, Azienda Ospedaliero Universitaria Careggi, Florence, Italy; and.
Blood Adv. 2018 Nov 13;2(21):2964-2972. doi: 10.1182/bloodadvances.2018026245.
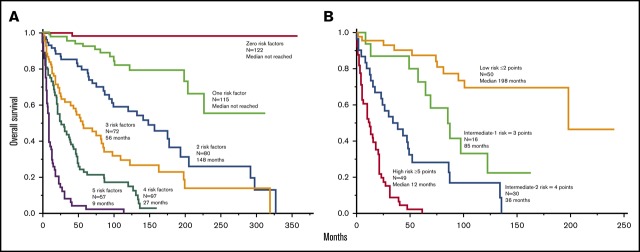
Systemic mastocytosis (SM) is a clinically heterogeneous disease with prognosis chiefly assigned based on World Health Organization (WHO) morphologic subclassification. We assessed the feasibility of developing contemporary risk models for SM based on clinical and integrated clinical-genetics information. Diagnosis of SM was per WHO criteria, and karyotype and next-generation sequencing data were available in a subset of the total 580 patients (median age, 55 years; range, 18-88 years) seen at the Mayo Clinic between 1968 and 2015. Morphologic subcategories were indolent/smoldering in 291 (50%) and "advanced" in 289 (50%): SM with an associated hematological neoplasm in 199, aggressive SM in 85, and mast cell leukemia in 5. Multivariable analysis of clinical variables identified age >60 years, advanced SM, thrombocytopenia <150 × 10/L, anemia below sex-adjusted normal, and increased alkaline phosphatase (ALP) as independent risk factors for survival; respective hazard ratios (HRs) 95% confidence intervals (95% CIs) were 2.5 (1.9-3.4), 2.7 (1.8-4.0), 2.5 (1.9-3.4), 2.2 (1.6-3.1), and 2.1 (1.5-3.0). In addition, (HR, 4.5; 95% CI, 2.6-7.6), (HR, 4.3; 95% CI, 1.3-10.8), and (HR, 5.0, 95% CI, 1.5-13.2) mutations were independently associated with inferior survival. Combined clinical, cytogenetic, and molecular risk factor analysis confirmed the independent prognostic contribution of adverse mutations (2.6, 1.6-4.4), advanced SM (4.0, 1.8-10.0), thrombocytopenia (2.8, 1.7-4.5), increased ALP (2.1, 1.2-4.0), and age >60 years (2.2, 1.3-3.6). These data were subsequently used to develop clinical and hybrid clinical-molecular risk models. The current study advances 2 complementary risk models for SM and highlights the independent prognostic contribution of mutations.
系统性肥大细胞增多症 (SM) 是一种临床表现异质性疾病,其预后主要基于世界卫生组织 (WHO) 的形态学分类。我们评估了基于临床和综合临床遗传学信息开发当代 SM 风险模型的可行性。SM 的诊断符合 WHO 标准,在梅奥诊所 1968 年至 2015 年间就诊的 580 例患者中(中位年龄 55 岁,范围 18-88 岁),有一部分患者的核型和下一代测序数据可用。形态学亚类为惰性/冒烟型 291 例(50%)和“进展型”289 例(50%):199 例伴有血液系统恶性肿瘤,85 例侵袭性 SM,5 例肥大细胞白血病。对临床变量的多变量分析确定年龄 >60 岁、进展型 SM、血小板计数 <150×10/L、贫血低于性别调整正常值和碱性磷酸酶(ALP)升高为生存的独立危险因素;相应的危险比(HR)95%置信区间(95%CI)分别为 2.5(1.9-3.4)、2.7(1.8-4.0)、2.5(1.9-3.4)、2.2(1.6-3.1)和 2.1(1.5-3.0)。此外, (HR,4.5;95%CI,2.6-7.6)、 (HR,4.3;95%CI,1.3-10.8)和 (HR,5.0,95%CI,1.5-13.2)突变与预后不良独立相关。综合临床、细胞遗传学和分子危险因素分析证实了不良突变(2.6,1.6-4.4)、进展型 SM(4.0,1.8-10.0)、血小板减少症(2.8,1.7-4.5)、ALP 升高(2.1,1.2-4.0)和年龄 >60 岁(2.2,1.3-3.6)的独立预后贡献。这些数据随后被用于开发临床和混合临床分子风险模型。本研究提出了两种互补的 SM 风险模型,并强调了突变的独立预后贡献。