Department of Oncology, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
The Sidney Kimmel Cancer Center, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
J Immunother Cancer. 2018 Nov 13;6(1):118. doi: 10.1186/s40425-018-0435-6.
The pancreatic cancer vaccine, GVAX, induces novel lymphoid aggregates in the otherwise immune quiescent pancreatic ductal adenocarcinoma (PDAC). GVAX also upregulates the PD-1/PD-L1 pathway, and a pre-clinical model demonstrated the anti-tumor effects of combination GVAX and anti-PD-1 antibody therapy (GVAX/αPD-1). Resistance to GVAX was associated with an immune-suppressive myeloid cell infiltration, which may limit further therapeutic gains of GVAX/αPD-1 therapy. The expression of CSF-1R, a receptor important for myeloid cell migration, differentiation and survival, and the effect of its therapeutic blockade in the context of GVAX in PDAC has not been investigated.
Lymphoid aggregates appreciated in 24 surgically resected PDAC from patients who received one dose of neoadjuvant GVAX were analyzed with multiplex immunohistochemistry. Flow cytometry analysis of tumor infiltrating T-cells in a murine model of PDAC was performed to investigate the therapeutic effects and mechanism of anti-CSF-1R/anti-PD-1/GVAX combination immunotherapy.
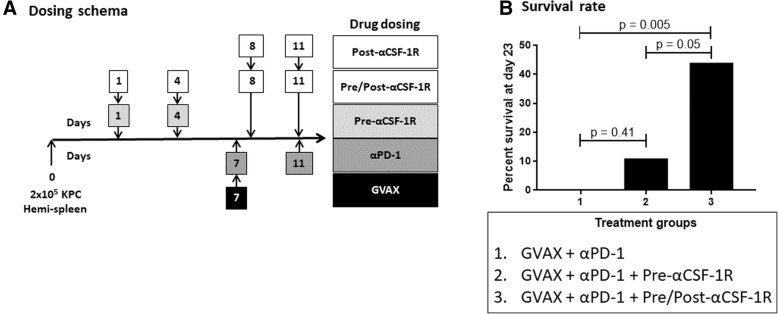
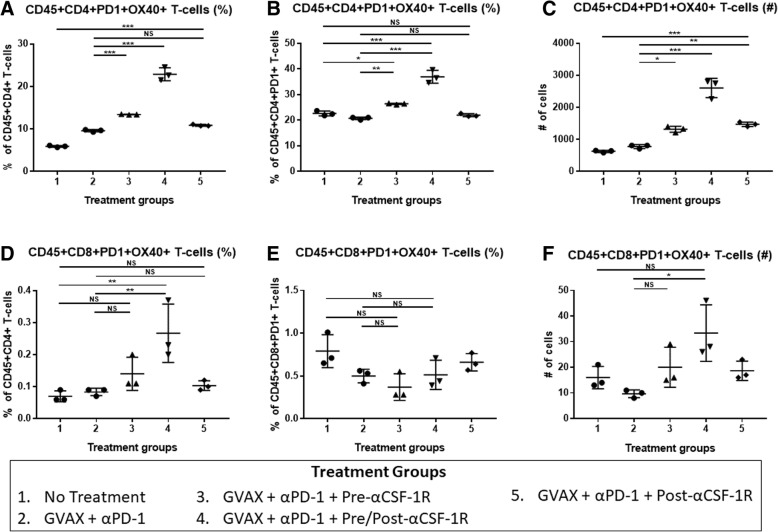
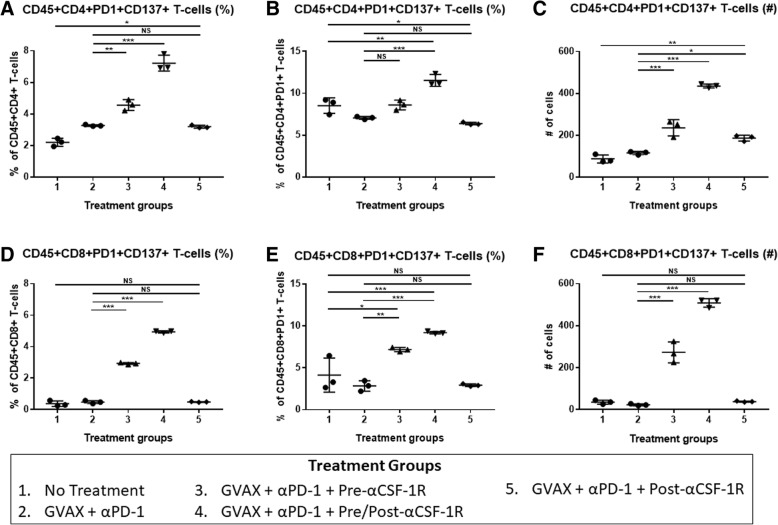
High CSF-1R expression in resected PDAC from patients who received neoadjuvant GVAX was associated with a higher myeloid to lymphoid cell ratio (p < 0.05), which has been associated with poorer survival. This higher CSF-1R expression was associated with a higher intra-tumoral infiltration of immature dendritic cells (p < 0.05), but not mature dendritic cells (p = 0.132). In the pre-clinical murine model, administering anti-CSF-1R antibody prior to and after GVAX/αPD-1 ("pre/post-αCSF-1R + αPD-1 + GVAX") enhanced the survival rate compared to GVAX/αPD-1 dual therapy (p = 0.005), but administering anti-CSF-1R only before GVAX/αPD-1 did not (p = 0.41). The "pre/post-αCSF-1R + αPD-1 + GVAX" group also had higher intra-tumoral infiltration of PD-1 + CD8+ and PD-1 + CD4+ T-cells compared to αPD-1/GVAX (p < 0.001). Furthermore, this regimen increased the intra-tumoral infiltration of PD-1 + CD137 + CD8+, PD-1 + CD137 + CD4+ and PD-1 + OX40 + CD4+ T-cells (p < 0.001). These PD-1 + CD137 + CD8+ T-cells expressed high levels of interferon-γ (median 80-90%) in response to stimulation with CD3/CD28 activation beads, and this expression was higher than that of PD-1 + CD137-CD8+ T-cells (p < 0.001).
The conversion of exhausted PD-1+ T-cells to CD137+ activated effector T-cells may contribute to the anti-tumor effects of the anti-CSF-1R/anti-PD-1/GVAX combination therapy. Anti-CSF-1R antibody with anti-PD-1 antibody and GVAX have the potential be an effective therapeutic strategy for treatment of PDAC.
胰腺癌疫苗 GVAX 可在原本免疫静止的胰腺导管腺癌(PDAC)中诱导新的淋巴聚集。GVAX 还上调了 PD-1/PD-L1 通路,临床前模型表明 GVAX 和抗 PD-1 抗体联合治疗(GVAX/αPD-1)具有抗肿瘤作用。对 GVAX 的耐药性与免疫抑制性髓样细胞浸润有关,这可能限制了 GVAX/αPD-1 治疗的进一步疗效。CSF-1R 的表达,一种对髓样细胞迁移、分化和存活很重要的受体,以及其在 GVAX 治疗 PDAC 中的治疗阻断作用尚未被研究。
对接受过一次新辅助 GVAX 治疗的 24 例手术切除的 PDAC 患者的淋巴聚集物进行了多重免疫组化分析。对 PDAC 的小鼠模型进行了肿瘤浸润性 T 细胞的流式细胞术分析,以研究抗 CSF-1R/抗 PD-1/GVAX 联合免疫治疗的治疗效果和机制。
接受新辅助 GVAX 治疗的 PDAC 患者中高 CSF-1R 表达与更高的髓样细胞与淋巴样细胞比值相关(p<0.05),这与生存率降低有关。这种高 CSF-1R 表达与肿瘤内不成熟树突状细胞的更高浸润相关(p<0.05),但与成熟树突状细胞无关(p=0.132)。在临床前的小鼠模型中,在 GVAX/αPD-1 之前和之后给予抗 CSF-1R 抗体(“pre/post-αCSF-1R + αPD-1 + GVAX”)与 GVAX/αPD-1 双重治疗相比提高了生存率(p=0.005),但仅在 GVAX/αPD-1 之前给予抗 CSF-1R 抗体则没有(p=0.41)。“pre/post-αCSF-1R + αPD-1 + GVAX”组与 αPD-1/GVAX 相比,肿瘤内 PD-1+CD8+和 PD-1+CD4+T 细胞的浸润也更高(p<0.001)。此外,该方案增加了肿瘤内 PD-1+CD137+CD8+、PD-1+CD137+CD4+和 PD-1+OX40+CD4+T 细胞的浸润(p<0.001)。这些 PD-1+CD137+CD8+T 细胞在与 CD3/CD28 激活珠刺激时表达高水平的干扰素-γ(中位数 80-90%),并且表达水平高于 PD-1+CD137-CD8+T 细胞(p<0.001)。
将耗尽的 PD-1+T 细胞转化为 CD137+激活的效应 T 细胞可能有助于抗 CSF-1R/抗 PD-1/GVAX 联合治疗的抗肿瘤作用。抗 CSF-1R 抗体与抗 PD-1 抗体和 GVAX 有可能成为治疗 PDAC 的有效治疗策略。