Divisions of Endocrinology and Metabolism and Pediatric Endocrinology, Departments of Medicine and Pediatrics, University of California, San Francisco, United States.
Endocrine Research Unit, San Francisco Veterans Affairs Health Care System, Department of Medicine, University of California, San Francisco, United States.
Best Pract Res Clin Endocrinol Metab. 2018 Oct;32(5):609-619. doi: 10.1016/j.beem.2018.05.004. Epub 2018 May 26.
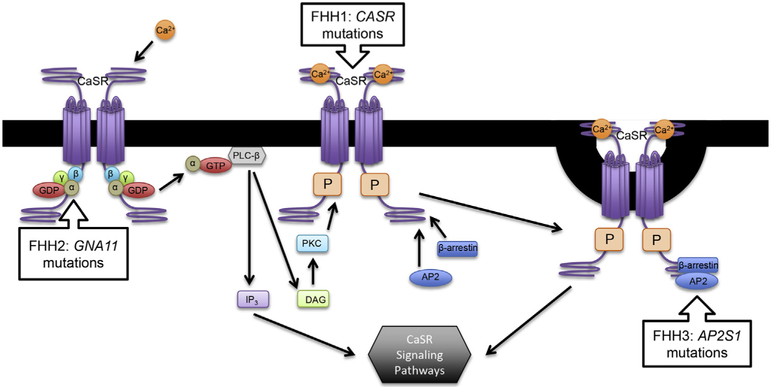
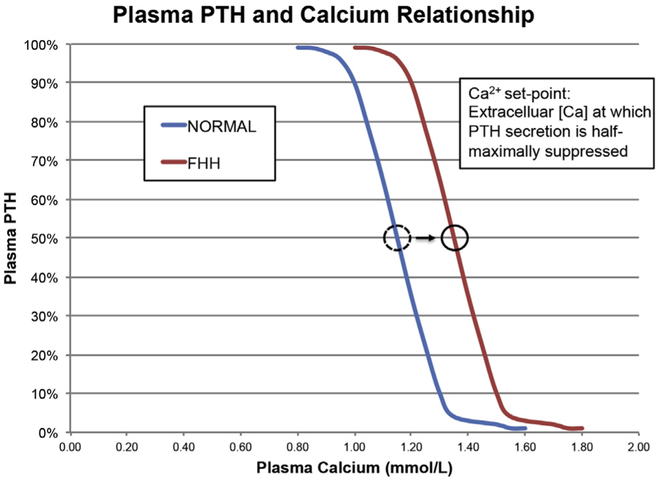
Familial hypocalciuric hypercalcemia (FHH) causes hypercalcemia by three genetic mechanisms: inactivating mutations in the calcium-sensing receptor, the G-protein subunit α, or adaptor-related protein complex 2, sigma 1 subunit. While hypercalcemia in other conditions causes significant morbidity and mortality, FHH generally follows a benign course. Failure to diagnose FHH can result in unwarranted treatment or surgery for the mistaken diagnosis of primary hyperparathyroidism (PHPT), given the significant overlap of biochemical features. Determinations of urinary calcium excretion greatly aid in distinguishing PHPT from FHH, but overlap still exists in certain cases. It is important that 24-h urine calcium and creatinine be included in the initial workup of hypercalcemia. FHH should be considered if low or even low normal urinary calcium levels are found in what is typically an asymptomatic hypercalcemic patient. The calcimimetic cinacalcet has been used to treat hypercalcemia in certain symptomatic causes of FHH.
家族性低钙血症性高钙血症(FHH)通过三种遗传机制引起高钙血症:钙敏感受体、G 蛋白亚基α或衔接蛋白相关复合物 2、sigma 1 亚基的失活突变。虽然其他情况下的高钙血症会导致严重的发病率和死亡率,但 FHH 通常呈良性过程。由于生化特征的显著重叠,未能诊断 FHH 可能导致对原发性甲状旁腺功能亢进症(PHPT)的误诊而进行不必要的治疗或手术。尿钙排泄的测定极大地有助于区分 PHPT 和 FHH,但在某些情况下仍存在重叠。在高钙血症的初始检查中,应包括 24 小时尿钙和肌酐。如果在典型无症状高钙血症患者中发现低甚至正常低水平的尿钙,则应考虑 FHH。在某些 FHH 的有症状病因中,钙敏感受体激动剂西那卡塞已被用于治疗高钙血症。