Cancer Biology Research Platform, Centre Georges-François Leclerc, Dijon, France.
Université de Bourgogne-Franche comté, Faculté des Sciences de Santé, Dijon, France.
J Immunother Cancer. 2018 Nov 19;6(1):123. doi: 10.1186/s40425-018-0438-3.
T lymphocytes and HLA expression on tumor cell both influence prognostic of localized colorectal cancer, but their role following chemotherapy in patients with liver metastatic colorectal cancer (mCRC) was not addressed.
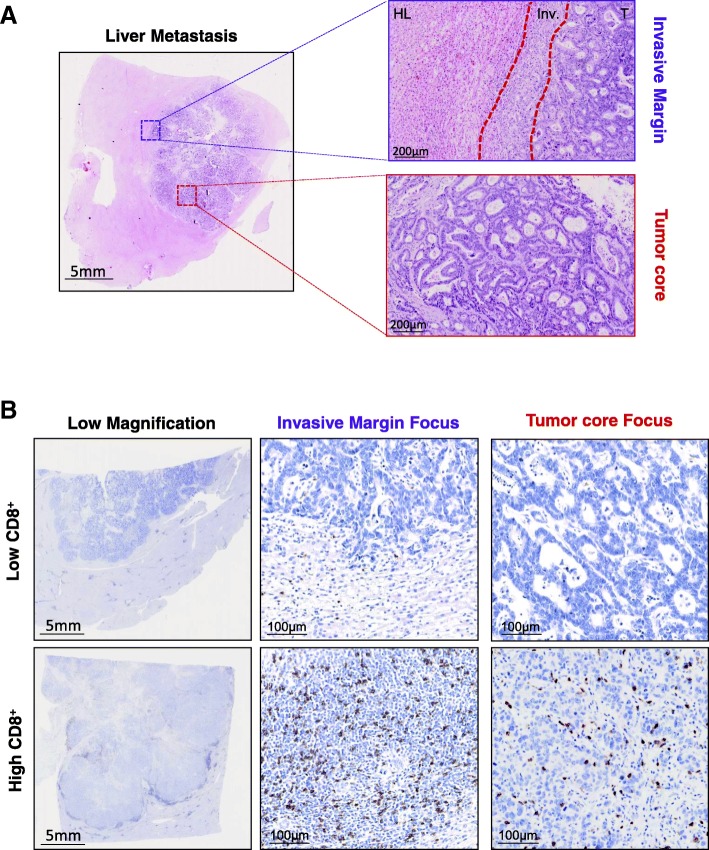
One hundred fourteen patients treated in curative intend of liver mCRC were included in this retrospective study. Patients were either untreated or treated with neoadjuvant therapy containing an anti-EGFR, bevacizumab or oxaliplatin. Immune densities were quantified in the tumor core and in invasive margin of metastases, using Qupath software or a pathologist's quantification. CD8, NKp46, Foxp3, CD163, HLA, PD-L1 were analyzed and were correlated with progression free survival (PFS) and overall survival (OS) using multivariable Cox proportional hazards models.
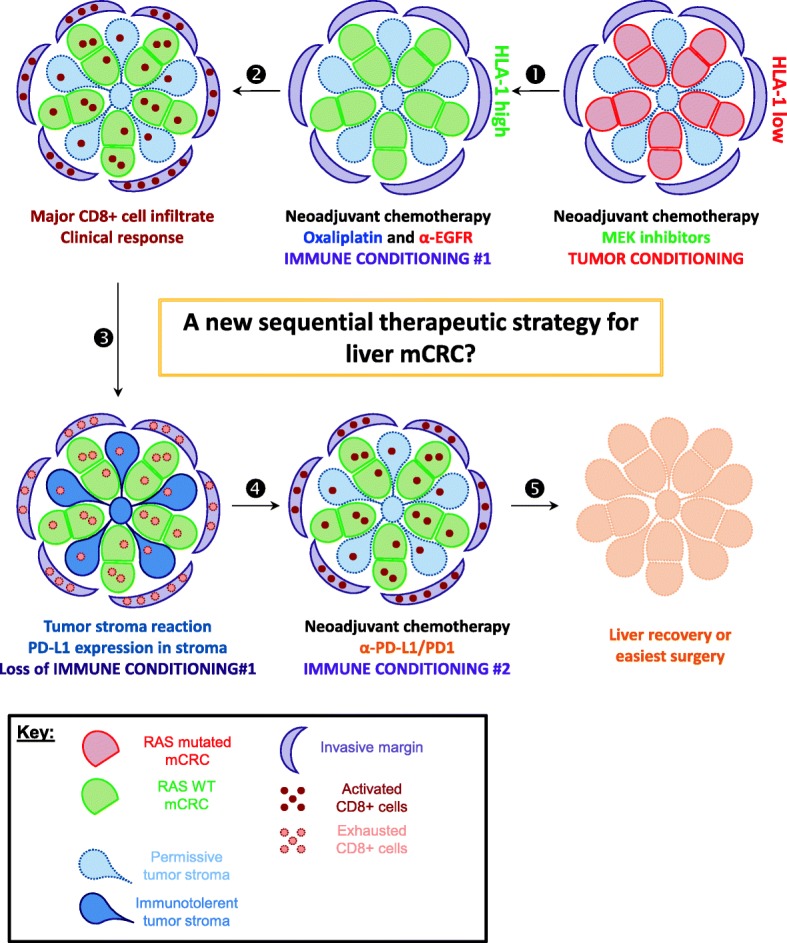
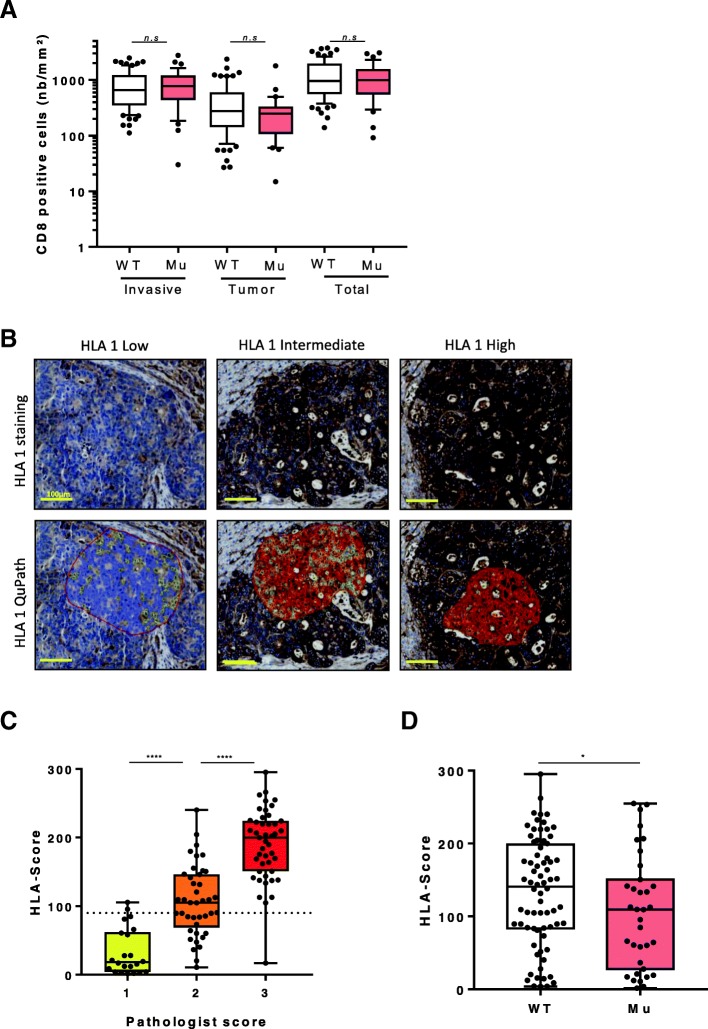
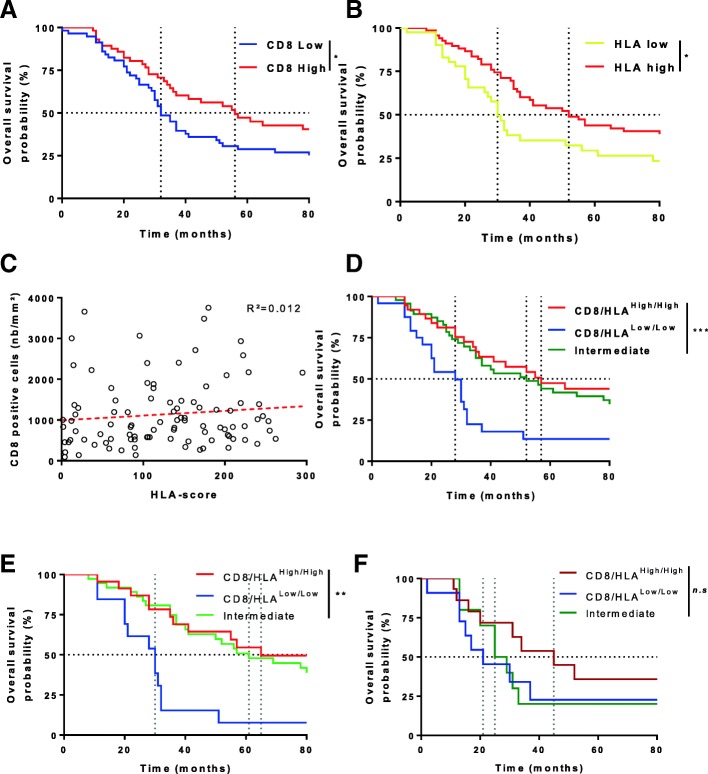
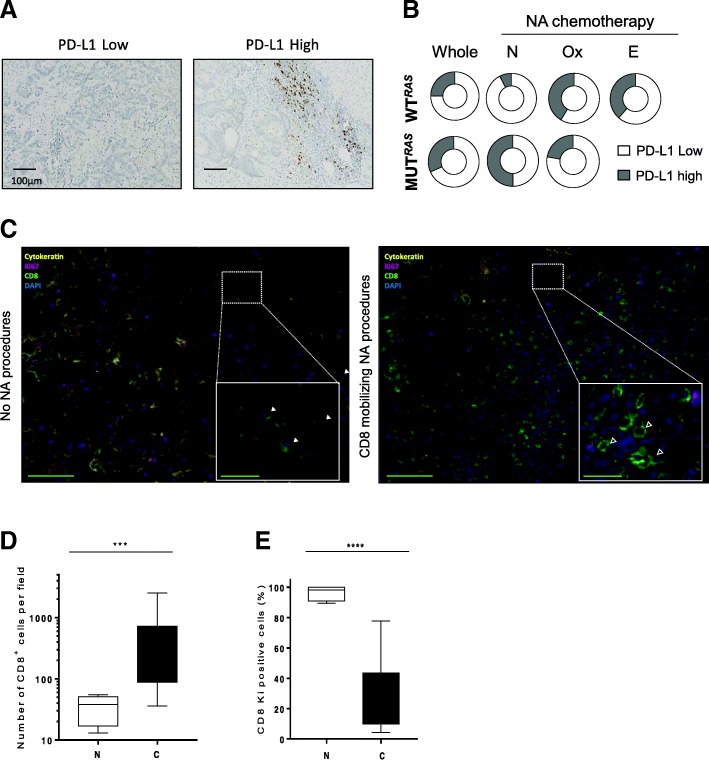
In the whole cohort only a high CD8+ cells infiltrate, a high HLA-I expression and wild-type RAS/RAF status were associated with a better overall survival in both univariate and multivariate model. Moreover, CD8+ cells immune infiltrate at invasive margin combined to HLA expression in cancer cell could increase patient's outcome prediction. RAS status but not immune cell infiltrate was associated with HLA expression on tumor cells. In comparison to untreated patients, neoadjuvant chemotherapy induced CD8+ cells recruitment and increased PD-L1 staining in immune infiltrates only for WT RAS patients. In this context, anti-EGFR and oxaliplatin based chemotherapy are the most powerful to induce CD8+ cells mobilization within the metastatic site.
While CD8 infiltrate and HLA expression appear to be prognostic for mCRC, CD8 and PD-L1 infiltrate are enhanced by neoadjuvant chemotherapy in mCRC under RAS status dependence.
T 淋巴细胞和肿瘤细胞上的 HLA 表达均影响局限性结直肠癌的预后,但它们在肝转移性结直肠癌(mCRC)患者化疗后的作用尚未得到解决。
本回顾性研究纳入了 114 例接受肝 mCRC 根治性治疗的患者。患者要么未接受治疗,要么接受了包含抗 EGFR、贝伐单抗或奥沙利铂的新辅助治疗。使用 Qupath 软件或病理学家的定量方法,在肿瘤核心和转移灶的浸润边缘定量免疫密度。分析 CD8、NKp46、Foxp3、CD163、HLA、PD-L1,并使用多变量 Cox 比例风险模型将其与无进展生存期(PFS)和总生存期(OS)相关联。
在整个队列中,只有高 CD8+细胞浸润、高 HLA-I 表达和野生型 RAS/RAF 状态与单变量和多变量模型中的总生存期改善相关。此外,肿瘤细胞中 CD8+细胞浸润与 HLA 表达的联合可以提高患者的预后预测。RAS 状态而不是免疫细胞浸润与肿瘤细胞上的 HLA 表达相关。与未接受治疗的患者相比,新辅助化疗仅诱导 WT RAS 患者的 CD8+细胞募集和增加免疫浸润中的 PD-L1 染色。在这种情况下,基于抗 EGFR 和奥沙利铂的化疗是最有力的诱导转移部位 CD8+细胞动员的方法。
虽然 CD8 浸润和 HLA 表达似乎对 mCRC 具有预后意义,但在 RAS 状态依赖性下,新辅助化疗可增强 mCRC 中的 CD8 和 PD-L1 浸润。