Department of Nephrology and Hypertension, Hannover Medical School, Carl-Neuberg-Strasse 1, 30625, Hannover, Germany.
Department of Hematology, Hemostasis, Oncology and Stem Cell Transplantation, Hannover Medical School, Hannover, Germany.
Crit Care. 2018 Nov 19;22(1):307. doi: 10.1186/s13054-018-2221-8.
Despite modern intensive care with standardized strategies against acute respiratory distress syndrome (ARDS), Pneumocystis pneumonia (PcP) remains a life-threatening disease with a high mortality rate. Here, we analyzed a large mixed cohort of immunocompromised patients with PcP, with regard to clinical course and treatment, and aimed at identifying predictors of outcome.
This was a single-center retrospective analysis in a tertiary care institution across 17 years. Diagnosis of PcP required typical clinical features and microbiological confirmation of Pneumocystis jirovecii. Epidemiological, clinical, laboratory and outcome data were collected from patient records.
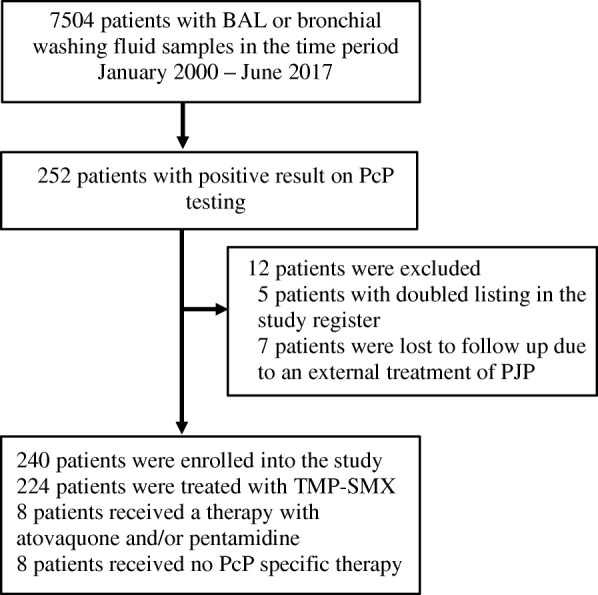
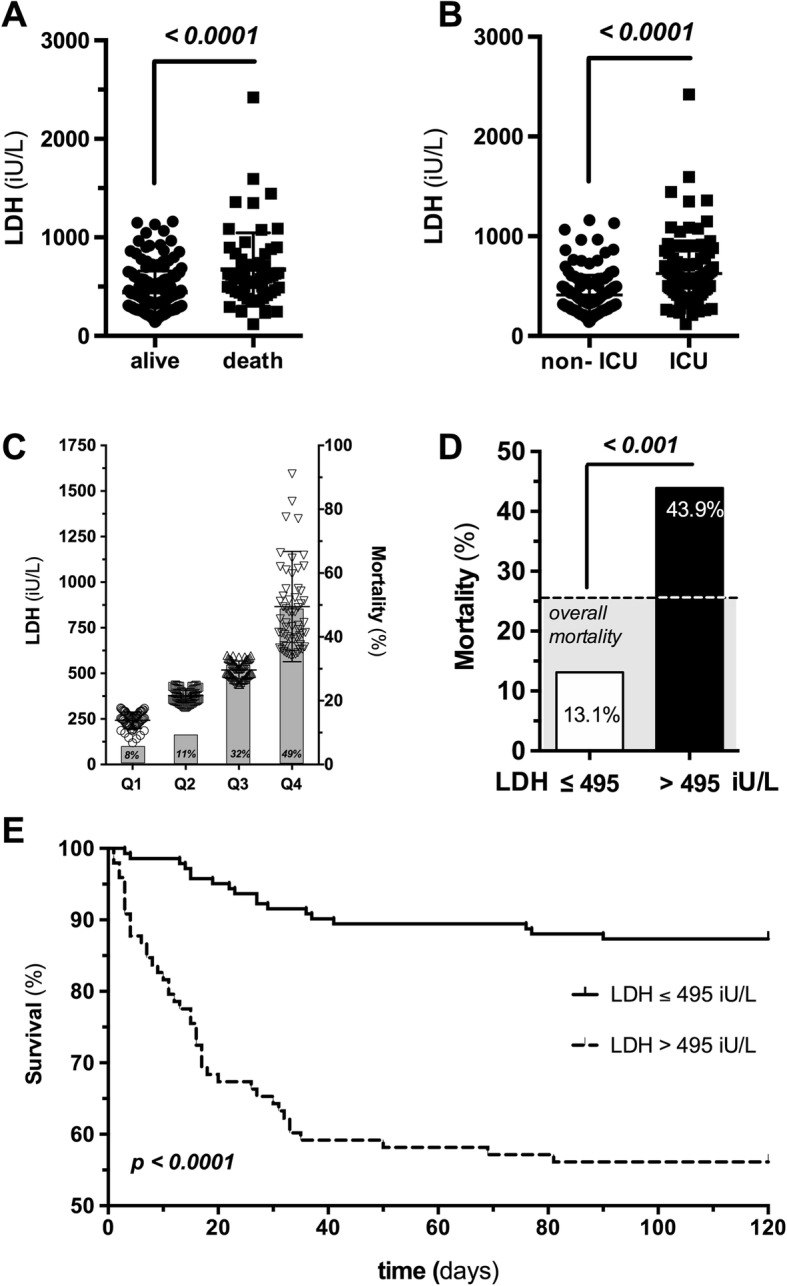
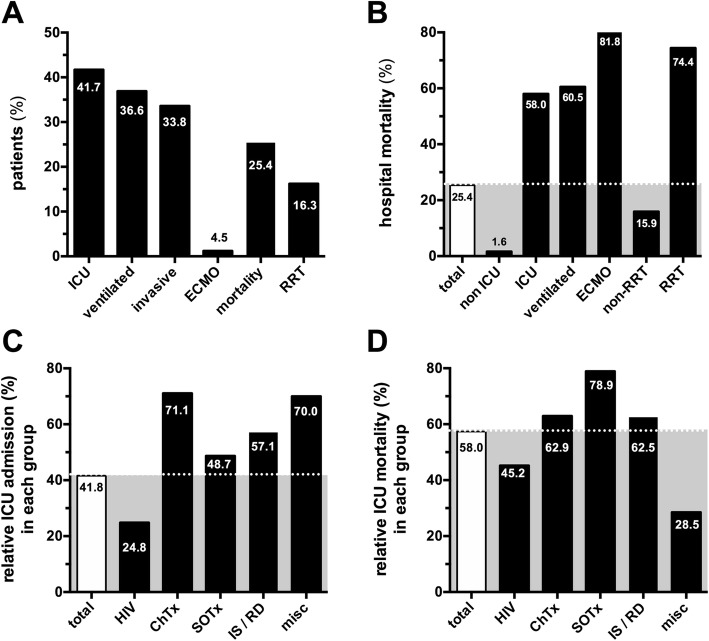
A total of 52,364 specimens from 7504 patients were sent for microbiological assessment (3653 with clinical suspicion of Pneumocystis pneumonia). PcP was confirmed in 240 patients, about half of them HIV positive (52%). The remaining subjects were either solid organ transplant recipients (16.3%) or suffered from malignancy (15.8%) or autoimmune diseases (11.7%). Of note, 95% of patients with PcP were not receiving chemoprophylaxis. Overall in-hospital mortality was 25.4%, increasing to 58% if ICU admission was required. Multivariable regression identified lactate dehydrogenase (LDH) as predictor of in-hospital mortality (adjusted OR 1.17 (95% CI 1.09-1.27), p < 0.0001). Mortality in LDH quartiles increased from 8% to 49%, and a cutoff value of 495 U/L predicted mortality with sensitivity and specificity of 70%. With regard to treatment, 40% of patients received trimethoprim-sulfamethoxazole at doses that were lower than recommended, and these patients had a higher mortality risk (HR 1.80 (95% CI 1.10-3.44), p = 0.02).
PcP remains a life-threatening disease among immunocompromised patients. About half of patients with PcP do not have HIV infection. Initial LDH values might serve as a stratifying tool to identify those patients at high risk of death among patients with HIV and without HIV infection.
尽管现代重症监护采用了针对急性呼吸窘迫综合征(ARDS)的标准化策略,但卡氏肺孢子菌肺炎(PcP)仍然是一种致命疾病,死亡率很高。在这里,我们分析了一组患有 PcP 的免疫功能低下患者的大型混合队列,以了解其临床过程和治疗方法,并旨在确定预后的预测因素。
这是一项在一家三级医疗机构进行的 17 年回顾性分析。PcP 的诊断需要典型的临床特征和卡氏肺孢子虫的微生物学确认。从患者记录中收集了流行病学、临床、实验室和结局数据。
共对 7504 名患者的 52364 份标本进行了微生物学评估(3653 份标本有卡氏肺孢子菌肺炎的临床怀疑)。240 名患者确诊为 PcP,其中约一半 HIV 阳性(52%)。其余患者为实体器官移植受者(16.3%)或患有恶性肿瘤(15.8%)或自身免疫性疾病(11.7%)。值得注意的是,95%的 PcP 患者未接受化学预防。总体院内死亡率为 25.4%,如果需要入住 ICU,则死亡率上升至 58%。多变量回归确定乳酸脱氢酶(LDH)为院内死亡率的预测因子(调整后的 OR 1.17(95%CI 1.09-1.27),p<0.0001)。LDH 四分位区间的死亡率从 8%增加到 49%,495U/L 的截断值预测死亡率的敏感性和特异性分别为 70%。关于治疗,40%的患者接受了低于推荐剂量的复方磺胺甲噁唑,这些患者的死亡率更高(HR 1.80(95%CI 1.10-3.44),p=0.02)。
PcP 仍然是免疫功能低下患者的一种危及生命的疾病。约一半的 PcP 患者没有 HIV 感染。初始 LDH 值可作为一种分层工具,用于识别 HIV 感染和无 HIV 感染患者中死亡风险较高的患者。