Chen Zhicai, Zhang Ruiting, Zhou Ying, Gong Xiaoxian, Zhang Meixia, Shi Feina, Yu Xinfeng, Lou Min
Department of Neurology, The Second Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China.
Department of Radiology, The Second Affiliated Hospital of Zhejiang University, School of Medicine, Hangzhou, China.
Front Neurol. 2018 Nov 5;9:933. doi: 10.3389/fneur.2018.00933. eCollection 2018.
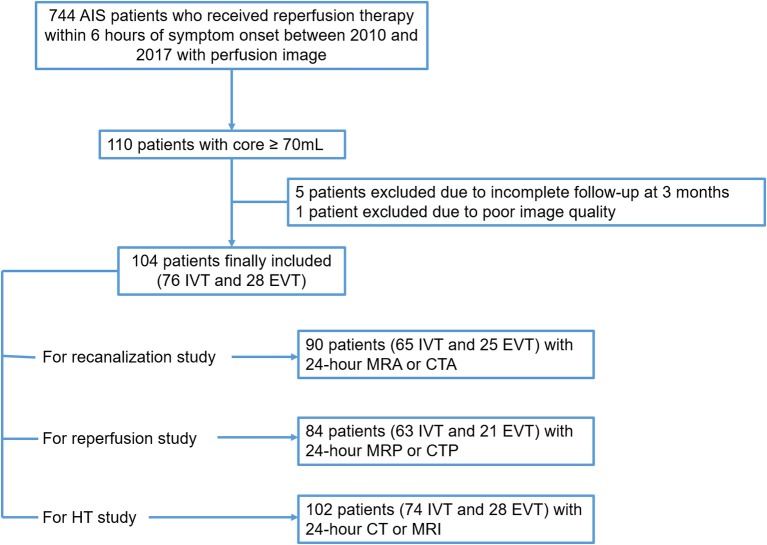
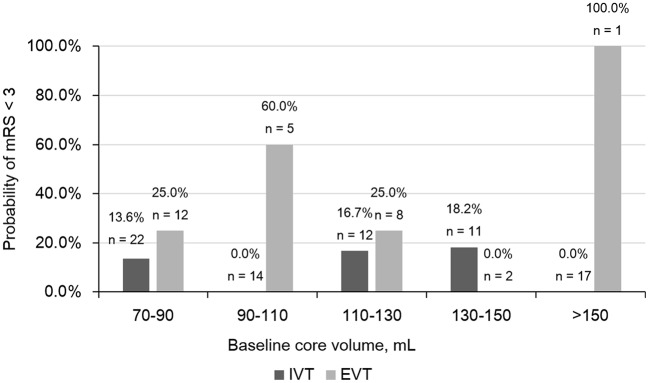
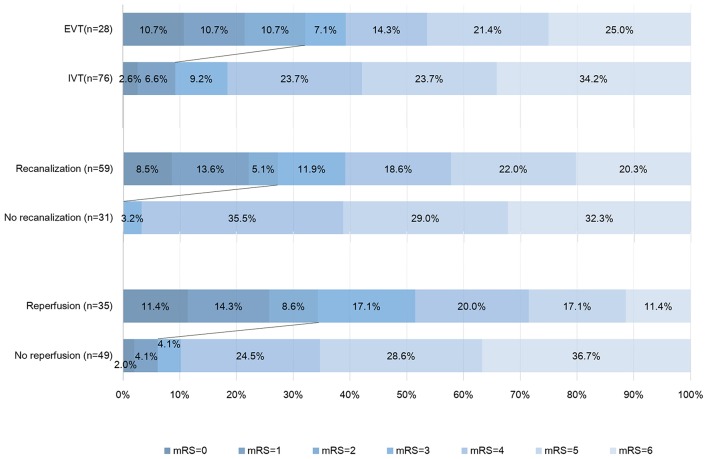
Large core is associated with poor outcome in acute ischemic stroke (AIS) patients. It is unclear whether endovascular treatment (EVT) could bring benefits to patients with core volume ≥70 ml before treatment. We aimed to compare the impact of EVT with intravenous thrombolysis (IVT) on the outcome in patients with core volume ≥70 ml. We included consecutive anterior circulation AIS patients who underwent MR or CT perfusion within 6 h post stroke onset, which revealed a core ≥70 ml before reperfusion therapy. Good outcome was defined by modified Rankin Scale of 0 to 2 at 90-day. Reperfusion was defined as a reduction in hypoperfusion volume of ≥70% between baseline and 24 h. One hundred four patients were included. Among them, 76 received IVT only, and 28 received EVT. After adjusting for age, NIHSS score, baseline core volume and onset to imaging time, patients in EVT group were more likely to achieve good outcome compared to IVT patients (OR, 3.875; 95% Cl 1.068-14.055, = 0.039). More patients in EVT group achieved recanalization (84.0 vs. 58.5%, = 0.027) and reperfusion (66.7 vs. 33.3%, = 0.010) than in IVT group. Reperfusion also independently predicted good outcome (OR, 7.718; 95% Cl 1.713-34.772, = 0.008). All patients with good outcome achieved recanalization at 24 h. Our data indicated that patients with core volume ≥70 ml might still benefit from EVT, which was related to its high reperfusion rate.
大面积梗死核心与急性缺血性卒中(AIS)患者的不良预后相关。目前尚不清楚血管内治疗(EVT)能否使治疗前梗死核心体积≥70 ml的患者获益。我们旨在比较EVT与静脉溶栓(IVT)对梗死核心体积≥70 ml患者预后的影响。我们纳入了卒中发作后6小时内接受磁共振成像(MR)或计算机断层扫描(CT)灌注检查的连续性前循环AIS患者,这些检查显示在再灌注治疗前梗死核心≥70 ml。良好预后定义为90天时改良Rankin量表评分为0至2分。再灌注定义为基线与24小时之间低灌注体积减少≥70%。共纳入104例患者。其中,76例仅接受IVT,28例接受EVT。在调整年龄、美国国立卫生研究院卒中量表(NIHSS)评分、基线梗死核心体积和发病至成像时间后,与IVT组患者相比,EVT组患者更有可能获得良好预后(比值比[OR],3.875;95%置信区间[Cl] 1.068 - 14.055,P = 0.039)。与IVT组相比,EVT组更多患者实现再通(84.0%对58.5%,P = 0.027)和再灌注(66.7%对33.3%,P = 0.010)。再灌注也独立预测良好预后(OR,7.718;95% Cl 1.713 - 34.772,P = 0.008)。所有预后良好的患者在24小时时均实现再通。我们的数据表明,梗死核心体积≥70 ml的患者可能仍能从EVT中获益,这与其高再灌注率有关。