Kerleroux Basile, Janot Kevin, Hak Jean François, Kaesmacher Johannes, Hassen Wagih Ben, Benzakoun Joseph, Oppenheim Catherine, Herbreteau Denis, Ifergan Heloise, Bricout Nicolas, Henon Hilde, Yoshimoto Takeshi, Inoue Manabu, Consoli Arturo, Costalat Vincent, Naggara Olivier, Lapergue Bertrand, Cagnazzo Federico, Boulouis Grégoire
Department of Neuroradiology, GHU Paris, Sainte Anne Hospital Pscyhiatry and Neurosciences Institute (IPNP), UMR_S1266, INSERM, University of Paris, Tours, France.
Department of Neuroradiology, University Hospital of Tours, Tours, France.
J Stroke. 2021 Sep;23(3):358-366. doi: 10.5853/jos.2021.00724. Epub 2021 Sep 30.
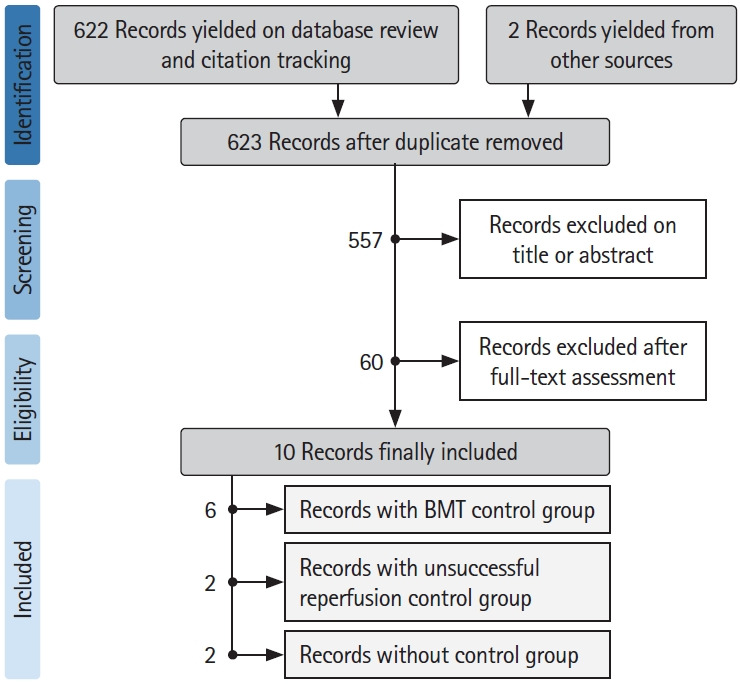
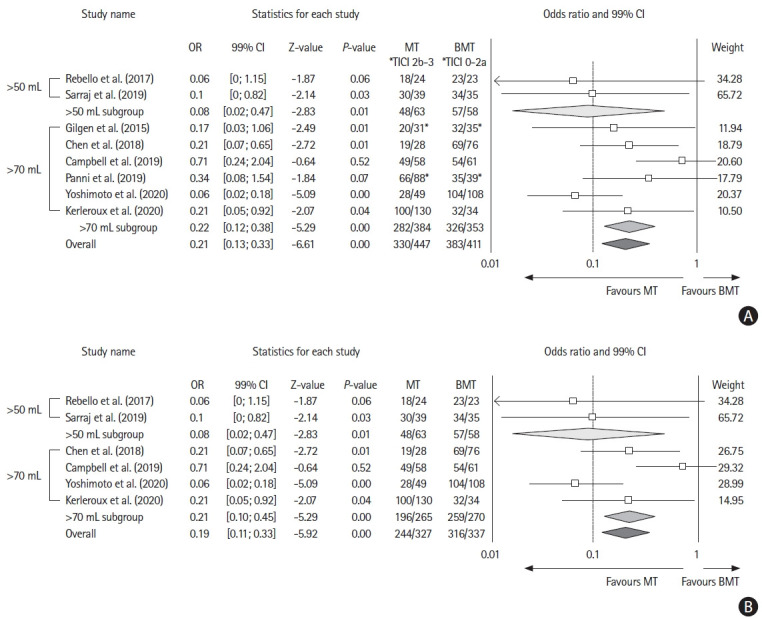
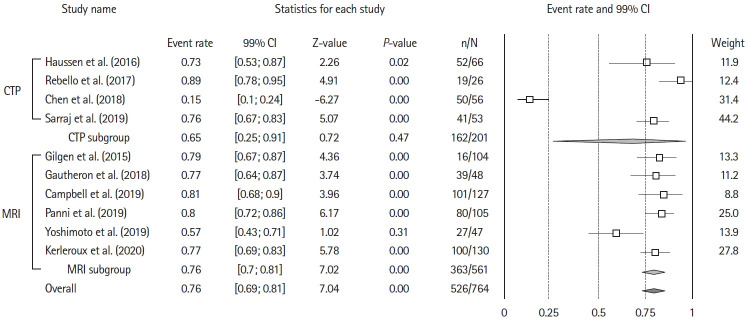
The benefits of mechanical thrombectomy (MT) for patients with acute ischemic stroke (AIS) and a large ischemic core (LIC) at presentation are uncertain. We aimed to obtain up-to-date aggregate estimates of the outcomes following MT in patients with volumetrically assessed LIC. We conducted a Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)-conformed, PROSPERO-registered, systematic review and meta-analysis of studies that included patients with AIS and a baseline LIC treated with MT, reported ischemic core volume quantitatively, and included patients with a LIC defined as a core volume ≥50 mL. The search was restricted to studies published between January 2015 and June 2020. Random-effects-meta-analysis was used to assess the effect of MT on 90-day unfavorable outcome (i.e., modified Rankin Scale [mRS] 3-6), mortality, and symptomatic intracranial hemorrhage (sICH) occurrence. Sensitivity analyses were performed for imaging-modality (computed tomography-perfusion or magnetic resonance-diffusion weighted imaging) and LIC-definition (≥50 or ≥70 mL). We analyzed 10 studies (954 patients), including six (682 patients) with a control group, allowing to compare 332 patients with MT to 350 who received best-medical-management alone. Overall, after MT the rate of patients with mRS 3-6 at 90 days was 74% (99% confidence interval [CI], 67 to 84; Z-value=7.04; I2=92.3%) and the rate of 90-day mortality was 36% (99% CI, 33 to 40; Z-value=-7.07; I2=74.5). Receiving MT was associated with a significant decrease in mRS 3-6 odds ratio (OR) 0.19 (99% CI, 0.11 to 0.33; P<0.01; Z-value=-5.92; I2=62.56) and in mortality OR 0.60 (99% CI, 0.34 to 1.06; P=0.02; Z-value=-2.30; I2=58.72). Treatment group did not influence the proportion of patients experiencing sICH, OR 0.96 (99% CI, 0.2 to 1.49; P=0.54; Z-value=-0.63; I2=64.74). Neither imaging modality for core assessment, nor LIC definition influenced the aggregated outcomes. Using aggregate estimates, MT appeared to decrease the risk of unfavorable functional outcome in patients with a LIC assessed volumetrically at baseline.
对于急性缺血性卒中(AIS)且就诊时存在大面积缺血核心(LIC)的患者,机械取栓(MT)的益处尚不确定。我们旨在获取对经体积评估的LIC患者进行MT后结局的最新综合估计。我们进行了一项遵循系统评价和Meta分析的首选报告项目(PRISMA)、在国际前瞻性系统评价注册库(PROSPERO)注册的系统评价和Meta分析,纳入了AIS且基线LIC接受MT治疗、定量报告缺血核心体积、且LIC定义为核心体积≥50 mL的患者的研究。检索限于2015年1月至2020年6月发表的研究。采用随机效应Meta分析评估MT对90天不良结局(即改良Rankin量表[mRS] 3 - 6)、死亡率和症状性颅内出血(sICH)发生情况的影响。针对成像方式(计算机断层扫描灌注或磁共振扩散加权成像)和LIC定义(≥50或≥70 mL)进行了敏感性分析。我们分析了10项研究(954例患者),其中6项(682例患者)有对照组,从而能够将332例接受MT的患者与350例仅接受最佳药物治疗的患者进行比较。总体而言,MT后90天mRS 3 - 6患者的比例为74%(99%置信区间[CI],67至84;Z值 = 7.04;I² = 92.3%),90天死亡率为36%(99% CI,33至40;Z值 = -7.07;I² = 74.5)。接受MT与mRS 3 - 6比值比(OR)显著降低相关,为0.19(99% CI,0.11至0.33;P < 0.01;Z值 = -5.92;I² = 62.56),死亡率OR为0.60(99% CI,0.34至1.06;P = 0.02;Z值 = -2.30;I² = 58.72)。治疗组不影响发生sICH患者的比例,OR为0.96(99% CI,0.2至1.49;P = 0.54;Z值 = -0.63;I² = 64.74)。核心评估的成像方式和LIC定义均不影响综合结局。使用综合估计,MT似乎降低了基线时经体积评估的LIC患者出现不良功能结局的风险。