Deep Medicine, Oxford Martin School, Oxford, United Kingdom.
The George Institute for Global Health, University of Oxford, Oxford, United Kingdom.
PLoS Med. 2018 Nov 20;15(11):e1002695. doi: 10.1371/journal.pmed.1002695. eCollection 2018 Nov.
Emergency admissions are a major source of healthcare spending. We aimed to derive, validate, and compare conventional and machine learning models for prediction of the first emergency admission. Machine learning methods are capable of capturing complex interactions that are likely to be present when predicting less specific outcomes, such as this one.
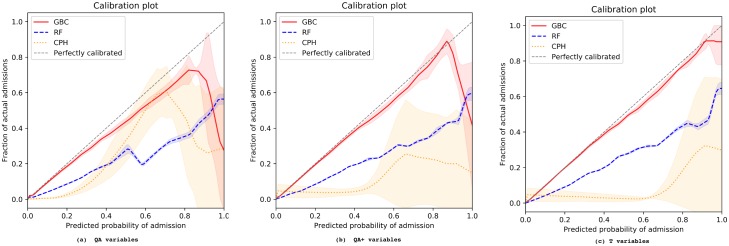
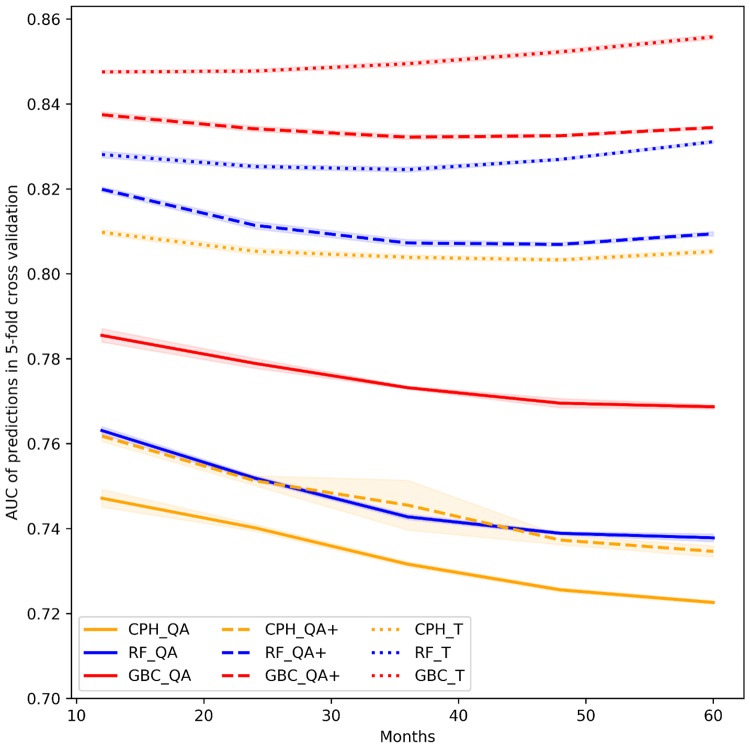
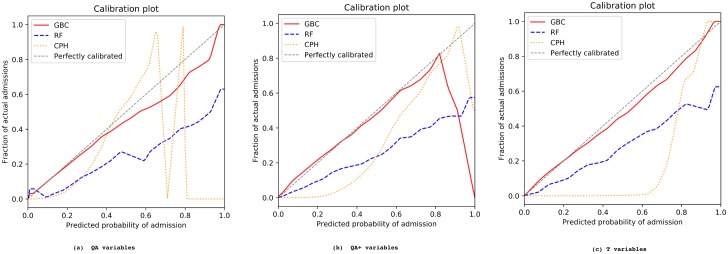
We used longitudinal data from linked electronic health records of 4.6 million patients aged 18-100 years from 389 practices across England between 1985 to 2015. The population was divided into a derivation cohort (80%, 3.75 million patients from 300 general practices) and a validation cohort (20%, 0.88 million patients from 89 general practices) from geographically distinct regions with different risk levels. We first replicated a previously reported Cox proportional hazards (CPH) model for prediction of the risk of the first emergency admission up to 24 months after baseline. This reference model was then compared with 2 machine learning models, random forest (RF) and gradient boosting classifier (GBC). The initial set of predictors for all models included 43 variables, including patient demographics, lifestyle factors, laboratory tests, currently prescribed medications, selected morbidities, and previous emergency admissions. We then added 13 more variables (marital status, prior general practice visits, and 11 additional morbidities), and also enriched all variables by incorporating temporal information whenever possible (e.g., time since first diagnosis). We also varied the prediction windows to 12, 36, 48, and 60 months after baseline and compared model performances. For internal validation, we used 5-fold cross-validation. When the initial set of variables was used, GBC outperformed RF and CPH, with an area under the receiver operating characteristic curve (AUC) of 0.779 (95% CI 0.777, 0.781), compared to 0.752 (95% CI 0.751, 0.753) and 0.740 (95% CI 0.739, 0.741), respectively. In external validation, we observed an AUC of 0.796, 0.736, and 0.736 for GBC, RF, and CPH, respectively. The addition of temporal information improved AUC across all models. In internal validation, the AUC rose to 0.848 (95% CI 0.847, 0.849), 0.825 (95% CI 0.824, 0.826), and 0.805 (95% CI 0.804, 0.806) for GBC, RF, and CPH, respectively, while the AUC in external validation rose to 0.826, 0.810, and 0.788, respectively. This enhancement also resulted in robust predictions for longer time horizons, with AUC values remaining at similar levels across all models. Overall, compared to the baseline reference CPH model, the final GBC model showed a 10.8% higher AUC (0.848 compared to 0.740) for prediction of risk of emergency admission within 24 months. GBC also showed the best calibration throughout the risk spectrum. Despite the wide range of variables included in models, our study was still limited by the number of variables included; inclusion of more variables could have further improved model performances.
The use of machine learning and addition of temporal information led to substantially improved discrimination and calibration for predicting the risk of emergency admission. Model performance remained stable across a range of prediction time windows and when externally validated. These findings support the potential of incorporating machine learning models into electronic health records to inform care and service planning.
急诊入院是医疗保健支出的主要来源。我们旨在开发、验证和比较传统和机器学习模型,以预测首次急诊入院。机器学习方法能够捕捉到在预测不太具体的结果(如本次预测)时可能存在的复杂交互作用。
我们使用来自英格兰 389 家实践中的 460 万名 18-100 岁患者的纵向电子健康记录数据,时间范围为 1985 年至 2015 年。该人群分为来自 300 家普通实践的 80%(375 万名患者)的推导队列和来自地理上不同、风险水平不同的 89 家普通实践的 20%(88 万名患者)的验证队列。我们首先复制了之前报告的用于预测基线后 24 个月内首次急诊入院风险的 Cox 比例风险(CPH)模型。然后将这个参考模型与两种机器学习模型(随机森林(RF)和梯度提升分类器(GBC))进行比较。所有模型的初始预测因子集包括 43 个变量,包括患者人口统计学、生活方式因素、实验室检查、目前开的药物、选择的合并症和之前的急诊入院情况。然后我们添加了 13 个变量(婚姻状况、之前的普通实践就诊情况和 11 个额外的合并症),并尽可能地通过纳入时间信息(例如,首次诊断后的时间)来丰富所有变量。我们还将预测窗口更改为基线后 12、36、48 和 60 个月,并比较了模型性能。对于内部验证,我们使用了 5 折交叉验证。当使用初始变量集时,GBC 的表现优于 RF 和 CPH,其接收者操作特征曲线(ROC)下面积(AUC)为 0.779(95%CI 0.777,0.781),分别为 0.752(95%CI 0.751,0.753)和 0.740(95%CI 0.739,0.741)。在外部验证中,我们观察到 GBC、RF 和 CPH 的 AUC 分别为 0.796、0.736 和 0.736。添加时间信息提高了所有模型的 AUC。在内部验证中,AUC 上升至 0.848(95%CI 0.847,0.849)、0.825(95%CI 0.824,0.826)和 0.805(95%CI 0.804,0.806),分别用于 GBC、RF 和 CPH,而外部验证的 AUC 上升至 0.826、0.810 和 0.788,分别用于 GBC、RF 和 CPH。这种增强还导致更长时间的预测具有稳健性,所有模型的 AUC 值保持在相似水平。总体而言,与基线参考 CPH 模型相比,最终的 GBC 模型在预测 24 个月内急诊入院风险方面的 AUC 提高了 10.8%(0.848 与 0.740 相比)。GBC 在整个风险范围内的校准效果也最好。尽管模型中包含了广泛的变量,但我们的研究仍然受到包含变量数量的限制;纳入更多的变量可以进一步提高模型性能。
机器学习的使用和时间信息的添加导致预测急诊入院风险的区分度和校准度有了显著提高。在一系列预测时间窗口和外部验证时,模型性能保持稳定。这些发现支持将机器学习模型纳入电子健康记录以提供护理和服务计划的潜力。