Centre for Evidence-Based Health Care, Division of Epidemiology and Biostatistics, Department of Global Health, Faculty of Medicine and Health Sciences, Stellenbosch University, Francie van Zijl drive, Parow, Cape Town, 7500, South Africa.
School of Public Health, College of Medicine and Health Science, University of Rwanda, Kicukiro, Kigali, Rwanda.
Syst Rev. 2018 Nov 20;7(1):203. doi: 10.1186/s13643-018-0865-8.
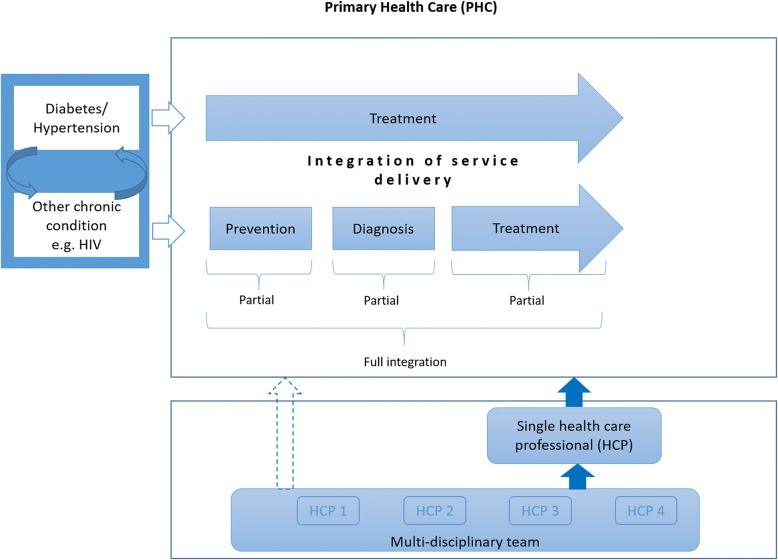
In low- and middle-income countries (LMICs), the burden of non-communicable diseases (NCDs) is growing against an existing burden of other diseases such as HIV/AIDS. Integrated models of care can help address the rising burden of multi-morbidity. Although integration of care can occur at various levels and has been defined in numerous ways, our aim is to assess the effects of integration of service delivery at primary healthcare level in LMICs.
We will consider randomised controlled trials (RCTs), cluster RCTs, non-randomised trials, controlled before-after studies and interrupted time series that examine integrated models of care among people with multi-morbidities, of which diabetes or hypertension is one, living in LMICs. We will compare fully integrated models of care to stand-alone care, partially integrated models of care to stand-alone care and fully integrated models to partially integrated models of care. Primary outcomes include all-cause mortality, disease-specific morbidity, HbA1c, systolic blood pressure and cholesterol levels. Secondary outcomes include access to care, retention in care, adherence, continuity of care, quality of care and cost of care. We will conduct a comprehensive search in the following databases: MEDLINE, EMBASE, the Cochrane Central Register of Control Trials, LILACS, Africa-Wide Information, CINAHL and Web of Science. In addition, we will search trial registries, relevant conference abstracts and check references lists of included studies. Selection of studies, data extraction and assessment of risk of bias will be performed independently by two review authors. We will resolve discrepancies through discussion with a third author. We will contact study authors in case of missing data. If included studies are sufficiently homogenous, we will pool results in a meta-analysis. Clinical heterogeneity related to the population, intervention, outcomes and context will be documented in table format and explored through subgroup analysis. We will assess χ and I tests for statistical heterogeneity. We will use GRADE to make judgements about the certainty of evidence and present findings in a summary of findings table.
In light of limited evidence on the provision of comprehensive care for diabetes and hypertension, and its comorbidity in LMCIs, we believe that the findings of this systematic review will provide a synthesis of evidence on effective models of integrated care for diabetes and hypertension and their comorbidities at primary healthcare level. This will enable policy-makers to device policies and programs that are evidence informed.
PROSPERO CRD42018099314 .
在中低收入国家(LMICs),非传染性疾病(NCDs)的负担正在增加,而艾滋病毒/艾滋病等其他疾病的负担也在增加。综合护理模式可以帮助应对多种疾病负担的增加。虽然护理整合可以在不同层面发生,并且已经有多种方式进行了定义,但我们的目标是评估在 LMICs 基层医疗保健层面提供服务的整合模式的效果。
我们将考虑随机对照试验(RCTs)、集群 RCTs、非随机试验、对照前后研究和中断时间序列,这些研究检查了中低收入国家患有多种疾病(其中一种为糖尿病或高血压)的人群的综合护理模式。我们将完全整合的护理模式与独立护理模式、部分整合的护理模式与独立护理模式、完全整合的护理模式与部分整合的护理模式进行比较。主要结果包括全因死亡率、特定疾病发病率、HbA1c、收缩压和胆固醇水平。次要结果包括获得护理的机会、护理保留率、依从性、护理连续性、护理质量和护理成本。我们将在以下数据库中进行全面搜索:MEDLINE、EMBASE、Cochrane 对照试验中心注册库、LILACS、非洲范围信息、CINAHL 和 Web of Science。此外,我们还将搜索试验注册处、相关会议摘要,并检查纳入研究的参考文献列表。两名综述作者将独立进行研究选择、数据提取和偏倚风险评估。我们将通过与第三位作者讨论来解决分歧。如果数据缺失,我们将联系研究作者。如果纳入的研究足够同质,我们将在荟萃分析中汇总结果。将以表格形式记录与人群、干预、结局和背景相关的临床异质性,并通过亚组分析进行探讨。我们将使用 χ 2 和 I 2 检验进行统计异质性评估。我们将使用 GRADE 对证据的确定性进行判断,并在总结发现表中呈现结果。
鉴于在 LMICs 中提供全面的糖尿病和高血压以及它们合并症的综合护理的证据有限,我们认为本系统评价的结果将综合糖尿病和高血压及其合并症在基层医疗保健层面的有效综合护理模式的证据。这将使决策者能够制定基于证据的政策和方案。
PROSPERO CRD42018099314 。