Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden.
Centre for Oncological Research, University of Antwerp, Antwerp, Belgium.
Genome Med. 2018 Nov 21;10(1):85. doi: 10.1186/s13073-018-0595-5.
There are multiple existing and emerging therapeutic avenues for metastatic prostate cancer, with a common denominator, which is the need for predictive biomarkers. Circulating tumor DNA (ctDNA) has the potential to cost-efficiently accelerate precision medicine trials to improve clinical efficacy and diminish costs and toxicity. However, comprehensive ctDNA profiling in metastatic prostate cancer to date has been limited.
A combination of targeted and low-pass whole genome sequencing was performed on plasma cell-free DNA and matched white blood cell germline DNA in 364 blood samples from 217 metastatic prostate cancer patients.
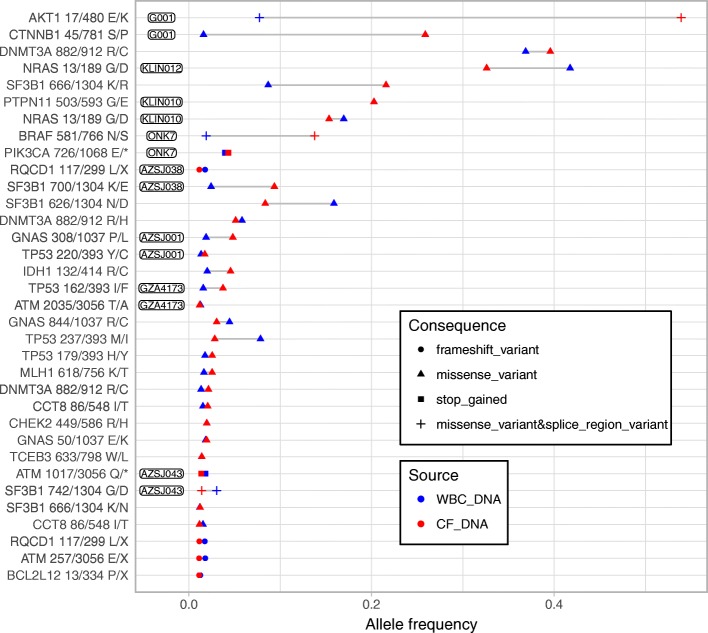
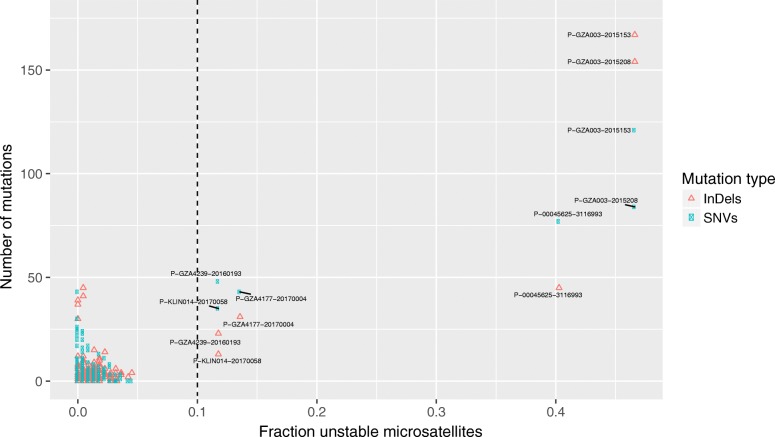
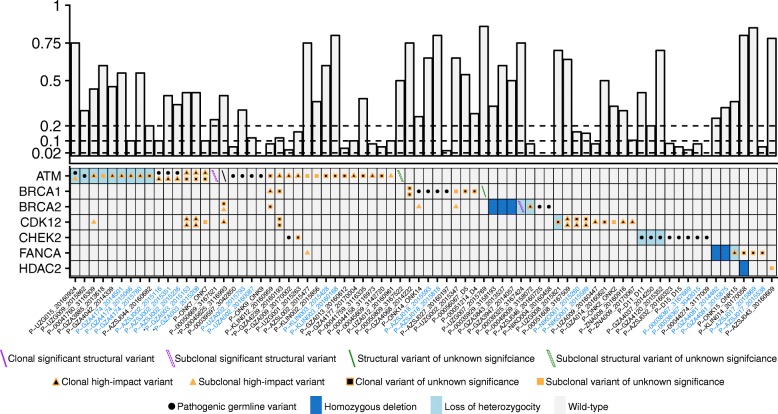
ctDNA was detected in 85.9% of baseline samples, correlated to line of therapy and was mirrored by circulating tumor cell enumeration of synchronous blood samples. Comprehensive profiling of the androgen receptor (AR) revealed a continuous increase in the fraction of patients with intra-AR structural variation, from 15.4% during first-line metastatic castration-resistant prostate cancer therapy to 45.2% in fourth line, indicating a continuous evolution of AR during the course of the disease. Patients displayed frequent alterations in DNA repair deficiency genes (18.0%). Additionally, the microsatellite instability phenotype was identified in 3.81% of eligible samples (≥ 0.1 ctDNA fraction). Sequencing of non-repetitive intronic and exonic regions of PTEN, RB1, and TP53 detected biallelic inactivation in 47.5%, 20.3%, and 44.1% of samples with ≥ 0.2 ctDNA fraction, respectively. Only one patient carried a clonal high-impact variant without a detectable second hit. Intronic high-impact structural variation was twice as common as exonic mutations in PTEN and RB1. Finally, 14.6% of patients presented false positive variants due to clonal hematopoiesis, commonly ignored in commercially available assays.
ctDNA profiles appear to mirror the genomic landscape of metastatic prostate cancer tissue and may cost-efficiently provide somatic information in clinical trials designed to identify predictive biomarkers. However, intronic sequencing of the interrogated tumor suppressors challenges the ubiquitous focus on coding regions and is vital, together with profiling of synchronous white blood cells, to minimize erroneous assignments which in turn may confound results and impede true associations in clinical trials.
转移性前列腺癌有多种现有的和新兴的治疗方法,它们有一个共同点,就是需要预测性生物标志物。循环肿瘤 DNA(ctDNA)有可能以具有成本效益的方式加速精准医学试验,以提高临床疗效,降低成本和毒性。然而,迄今为止,对转移性前列腺癌的全面 ctDNA 分析受到限制。
对 217 名转移性前列腺癌患者的 364 份血液样本中的血浆无细胞 DNA 和匹配的白细胞种系 DNA 进行了靶向和低深度全基因组测序的组合分析。
基线样本中 85.9%检测到 ctDNA,与治疗线相关,并与同步血液样本中循环肿瘤细胞计数相吻合。对雄激素受体(AR)的全面分析显示,具有 AR 内结构变异的患者比例不断增加,从一线转移性去势抵抗性前列腺癌治疗的 15.4%增加到四线的 45.2%,表明 AR 在疾病过程中的不断演变。患者经常发生 DNA 修复缺陷基因的改变(18.0%)。此外,在有资格的样本(≥0.1ctDNA 分数)中确定了微卫星不稳定性表型的 3.81%。对 PTEN、RB1 和 TP53 的非重复内含子和外显子区域进行测序,检测到具有≥0.2ctDNA 分数的样本中分别有 47.5%、20.3%和 44.1%的样本存在双等位基因失活。只有一名患者携带无检测到第二个突变的克隆性高影响变异。PTEN 和 RB1 中的内含子高影响结构变异比外显子突变常见两倍。最后,由于克隆性造血,14.6%的患者出现假阳性变异,而这在商业上可用的检测中通常被忽略。
ctDNA 谱似乎反映了转移性前列腺癌组织的基因组景观,并可在旨在识别预测性生物标志物的临床试验中以具有成本效益的方式提供体细胞信息。然而,对所研究的肿瘤抑制因子的内含子测序挑战了普遍关注编码区域的方法,这对于与同步白细胞的分析一起,最大限度地减少错误分配至关重要,否则可能会混淆结果,并阻碍临床试验中的真正关联。