Skjørten Ingunn, Hilde Janne Mykland, Melsom Morten Nissen, Hisdal Jonny, Hansteen Viggo, Steine Kjetil, Humerfelt Sjur
Department of Pulmonary Medicine, LHL Hospital Gardermoen, Jessheim,
Faculty of Medicine, University of Oslo, Oslo,
Int J Chron Obstruct Pulmon Dis. 2018 Oct 31;13:3599-3610. doi: 10.2147/COPD.S161175. eCollection 2018.
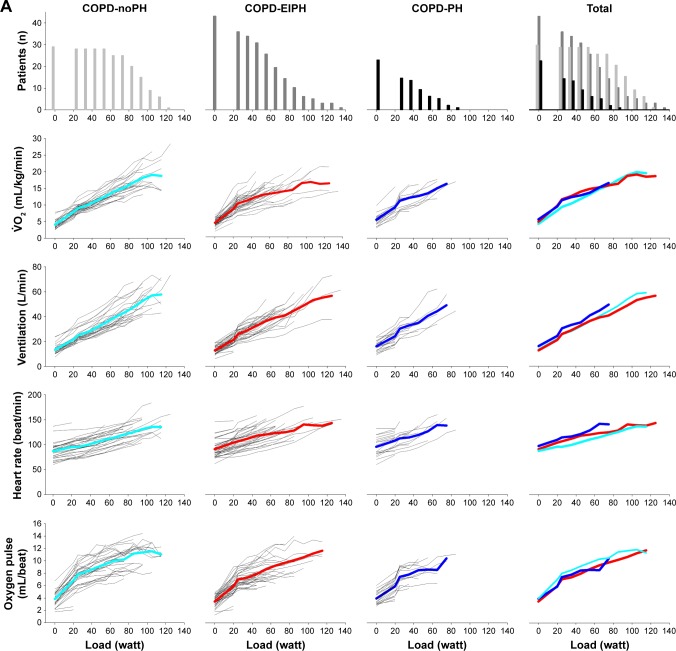
Pulmonary hypertension (PH) in patients with COPD is associated with reduced exercise capacity. A subgroup of COPD patients has normal mean pulmonary artery pressure (mPAP) at rest, but develops high mPAP relative to cardiac output (CO) during exercise, a condition we refer to as exercise-induced pulmonary hypertension (EIPH). We hypothesized that COPD patients with EIPH could be identified by cardiopulmonary exercise test (CPET) and that these patients have lower exercise capacity and more abnormal CPET parameters compared to COPD patients with normal hemodynamic exercise response.
Ninety-three stable outpatients with COPD underwent right heart catheterization with the measurement of mPAP, CO, and capillary wedge pressure at rest and during supine exercise. Resting mPAP <25 mmHg with ΔmPAP/ΔCO slope above or below 3 mmHg/L/min were defined as COPD-EIPH and COPD-normal, respectively. Pulmonary function tests and CPET with arterial blood gases were performed. Linear mixed models were fitted to estimate differences between the groups with adjustment for gender, age, and airflow obstruction.
EIPH was observed in 45% of the study population. Maximal workload was lower in COPD-EIPH compared to COPD-normal, whereas other CPET measurements at peak exercise in % predicted values were similar between the two groups. After adjustment for gender, age, and airflow obstruction, patients with COPD-EIPH showed significantly greater increase in oxygen uptake, ventilation, respiratory frequency, heart rate, and lactate with increasing work load, as well as more reduction in pH compared to those with normal hemodynamic responses.
COPD-EIPH could not be discriminated from COPD-normal by CPET. However, COPD-EIPH experienced a higher cost of exercise in terms of higher oxygen uptake, ventilation, respiratory frequency, heart rate, and lactate for a given increase in workload compared to COPD-normal.
慢性阻塞性肺疾病(COPD)患者的肺动脉高压(PH)与运动能力下降有关。一部分COPD患者静息时平均肺动脉压(mPAP)正常,但运动期间相对于心输出量(CO)会出现mPAP升高,我们将这种情况称为运动性肺动脉高压(EIPH)。我们推测,EIPH的COPD患者可通过心肺运动试验(CPET)来识别,并且与血流动力学运动反应正常的COPD患者相比,这些患者运动能力更低,CPET参数更异常。
93例稳定期COPD门诊患者接受了右心导管检查,测量静息和仰卧位运动时的mPAP、CO和毛细血管楔压。静息mPAP<25 mmHg且ΔmPAP/ΔCO斜率高于或低于3 mmHg/L/min分别定义为COPD-EIPH和COPD-正常。进行了肺功能测试和动脉血气CPET。采用线性混合模型估计两组之间的差异,并对性别、年龄和气流阻塞进行校正。
45%的研究人群观察到EIPH。与COPD-正常患者相比,COPD-EIPH患者的最大工作量更低,而两组在运动峰值时其他CPET测量的预测值百分比相似。在对性别、年龄和气流阻塞进行校正后,与血流动力学反应正常的患者相比,COPD-EIPH患者随着工作量增加,摄氧量、通气量、呼吸频率、心率和乳酸的增加明显更大,pH值下降也更多。
CPET无法区分COPD-EIPH和COPD-正常患者。然而,与COPD-正常患者相比,对于给定的工作量增加,COPD-EIPH患者在运动时以更高的摄氧量、通气量、呼吸频率、心率和乳酸为代价,运动成本更高。