Tremblay Gabriel, Dolph Mike, Bhor Menaka, Said Qayyim, Roy Anuja, Elliott Brian, Briggs Andrew
Health Economics, Purple Squirrel Economics, New York, NY, USA,
Health Economics and Outcomes Research, Novartis Pharmaceuticals, East Hanover, NJ, USA.
Clinicoecon Outcomes Res. 2018 Nov 5;10:715-721. doi: 10.2147/CEOR.S177338. eCollection 2018.
Immune thrombocytopenia (ITP) is an auto-immune disorder characterized by enhanced platelet destruction and, subsequently, the potential for increased bleeding. Thrombopoietin receptor (TPO-R) agonists have recently emerged as promising therapies for ITP patients who are refractory to other treatments. While eltrombopag (EPAG) is the only TPO-R agonist US Food and Drug Administration approved for use in pediatric patients, romiplostin (ROMI) has been used in Phase III clinical studies.
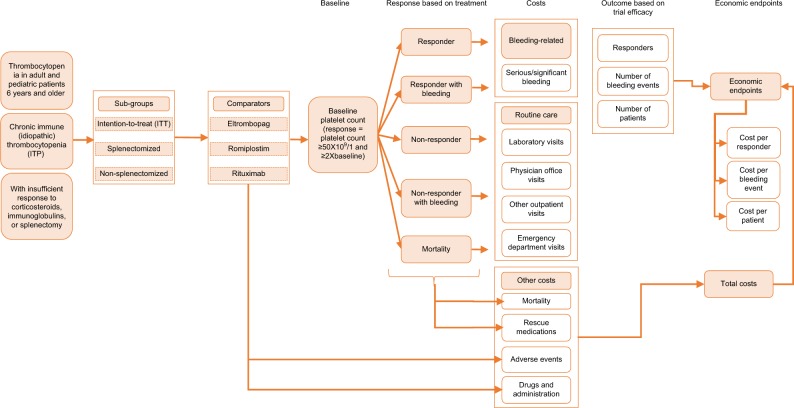
A cost-consequence model (CCM) was developed to evaluate the costs of EPAG, ROMI, and watch-and-rescue (W&R) in relation to their respective treatment outcomes in previously-treated pediatric chronic ITP (cITP) over a 26-week time horizon. The costs of drugs, administration, routine care, rescue medications, adverse events, and mortality were included. Data on platelet count response rate, bleeding events, and adverse events were derived from all relevant identified Phase III-registered clinical trials, health outcomes were compared via indirect treatment comparison.
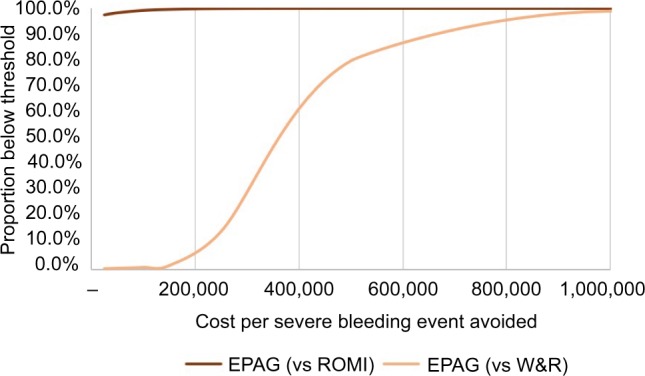
The overall estimated cost of EPAG per patient was US$66,550, compared to US$101,056 for ROMI and US$32,720 for W&R. EPAG's lower cost compared to ROMI was largely due to lower drug costs (US$62,202 vs US$84,396), administration costs (US$0 vs US$1,955), and significantly lower costs due to severe bleeding (US$354 vs US$10,191). When assessing cost per severe bleeding event avoided, EPAG was dominant over ROMI (less expensive and more effective). EPAG was again dominant over ROMI when assessing the cost per responder and per bleeding event (any grade). Sensitivity analysis was consistent with the base case findings.
EPAG was the preferred TPO-R agonist to treat cITP when indirectly compared to ROMI, largely driven by its favorable severe bleeding outcomes and lower drug and administration costs.
免疫性血小板减少症(ITP)是一种自身免疫性疾病,其特征是血小板破坏增强,进而有出血增加的风险。血小板生成素受体(TPO-R)激动剂最近已成为对其他治疗无效的ITP患者的有前景的治疗方法。虽然艾曲泊帕(EPAG)是美国食品药品监督管理局批准用于儿科患者的唯一TPO-R激动剂,但罗米司亭(ROMI)已用于III期临床研究。
建立了一个成本-后果模型(CCM),以评估EPAG、ROMI和观察与救援(W&R)在26周时间范围内,相对于先前治疗的儿童慢性ITP(cITP)各自治疗结果的成本。包括药物、给药、常规护理、救援药物、不良事件和死亡率的成本。血小板计数反应率、出血事件和不良事件的数据来自所有相关的已识别的III期注册临床试验,通过间接治疗比较来比较健康结果。
每位患者EPAG的总体估计成本为66,550美元,而ROMI为101,056美元,W&R为32,720美元。与ROMI相比,EPAG成本较低主要是由于药物成本较低(62,202美元对84,396美元)、给药成本较低(0美元对1,955美元)以及严重出血导致的成本显著较低(354美元对10,191美元)。在评估避免每例严重出血事件的成本时,EPAG优于ROMI(成本更低且更有效)。在评估每例缓解者和每例出血事件(任何级别)的成本时,EPAG再次优于ROMI。敏感性分析与基础病例结果一致。
与ROMI间接比较时,EPAG是治疗cITP的首选TPO-R激动剂,这主要是由其良好的严重出血结果以及较低的药物和给药成本所驱动。