Lawrence David S, Youssouf Nabila, Molloy Síle F, Alanio Alexandre, Alufandika Melanie, Boulware David R, Boyer-Chammard Timothée, Chen Tao, Dromer Francoise, Hlupeni Admire, Hope William, Hosseinipour Mina C, Kanyama Cecilia, Lortholary Oliver, Loyse Angela, Meya David B, Mosepele Mosepele, Muzoora Conrad, Mwandumba Henry C, Ndhlovu Chiratidzo E, Niessen Louis, Schutz Charlotte, Stott Katharine E, Wang Duolao, Lalloo David G, Meintjes Graeme, Jaffar Shabbar, Harrison Thomas S, Jarvis Joseph N
Department of Clinical Research, Faculty of Infectious and Tropical Diseases, London School of Hygiene and Tropical Medicine, London, UK.
Botswana-Harvard AIDS Institute Partnership, Gaborone, Botswana.
Trials. 2018 Nov 23;19(1):649. doi: 10.1186/s13063-018-3026-4.
Cryptococcal meningitis (CM) is a major cause of mortality in HIV programmes in Africa despite increasing access to antiretroviral therapy (ART). Mortality is driven in part by limited availability of amphotericin-based treatment, drug-induced toxicities of amphotericin B deoxycholate and prolonged hospital admissions. A single, high-dose of liposomal amphotericin (L-AmB, Ambisome) on a fluconazole backbone has been reported as non-inferior to 14 days of standard dose L-AmB in reducing fungal burden. This trial examines whether single, high-dose L-AmB given with high-dose fluconazole and flucytosine is non-inferior to a seven-day course of amphotericin B deoxycholate plus flucytosine (the current World Health Organization [WHO] recommended treatment regimen).
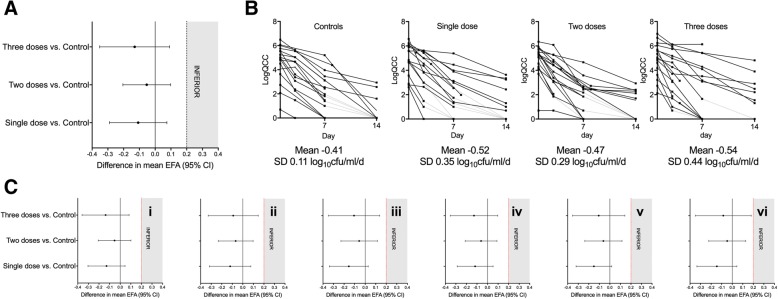
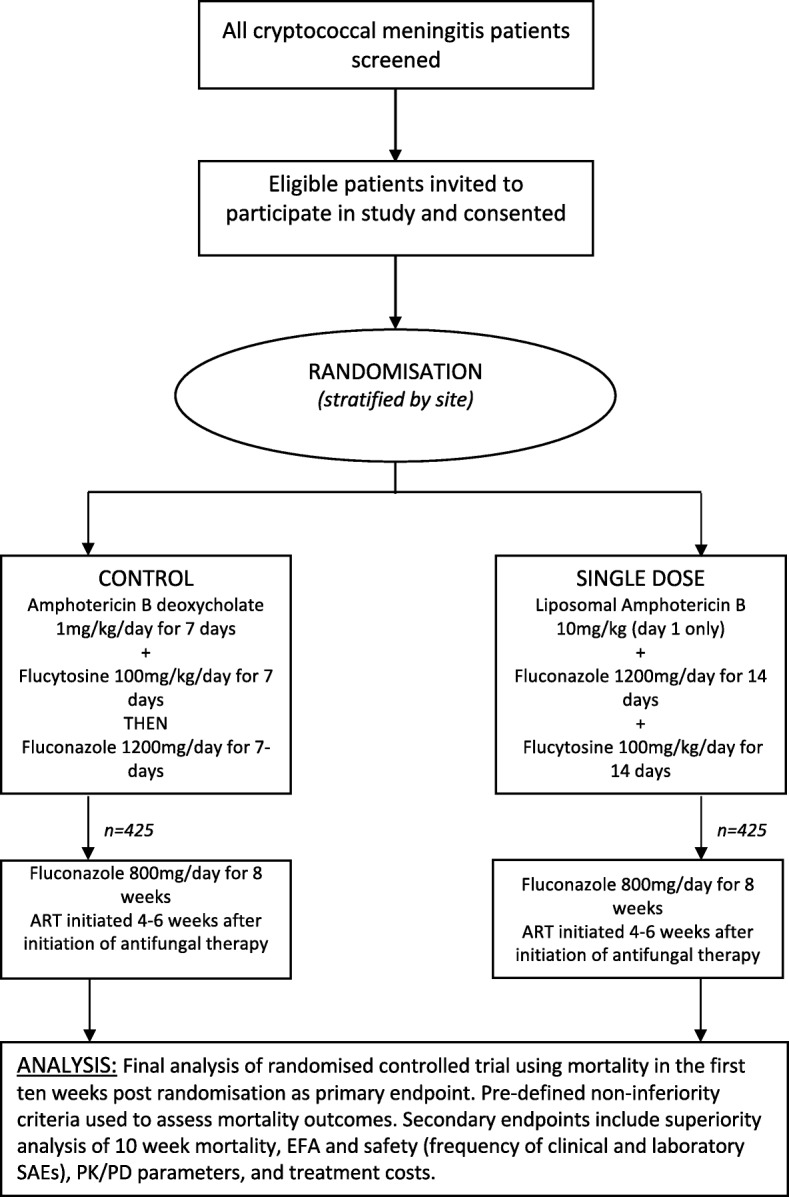
An open-label phase III randomised controlled non-inferiority trial conducted in five countries in sub-Saharan Africa: Botswana, Malawi, South Africa, Uganda and Zimbabwe. The trial will compare CM induction therapy with (1) a single dose (10 mg/kg) of L-AmB given with 14 days of fluconazole (1200 mg/day) and flucytosine (100 mg/kg/day) to (2) seven days amphotericin B deoxycholate (1 mg/kg/day) given alongside seven days of flucytosine (100 mg/kg/day) followed by seven days of fluconazole (1200 mg/day). The primary endpoint is all-cause mortality at ten weeks with a non-inferiority margin of 10% and 90% power. Secondary endpoints are early fungicidal activity, proportion of grade III/IV adverse events, pharmacokinetic parameters and pharmacokinetic/pharmacodynamic associations, health service costs, all-cause mortality within the first two and four weeks, all-cause mortality within the first ten weeks (superiority analysis) and rates of CM relapse, immune reconstitution inflammatory syndrome and disability at ten weeks. A total of 850 patients aged ≥ 18 years with a first episode of HIV-associated CM will be enrolled (425 randomised to each arm). All patients will be followed for 16 weeks. All patients will receive consolidation therapy with fluconazole 800 mg/day to complete ten weeks of treatment, followed by fluconazole maintenance and ART as per local guidance.
A safe, sustainable and easy to administer regimen of L-AmB that is non-inferior to seven days of daily amphotericin B deoxycholate therapy may reduce the number of adverse events seen in patients treated with amphotericin B deoxycholate and shorten hospital admissions, providing a highly favourable and implementable alternative to the current WHO recommended first-line treatment.
ISRCTN, ISRCTN72509687 . Registered on 13 July 2017.
尽管抗逆转录病毒疗法(ART)的可及性不断提高,但隐球菌性脑膜炎(CM)仍是非洲艾滋病项目中导致死亡的主要原因。死亡率部分归因于两性霉素类治疗药物供应有限、两性霉素B脱氧胆酸盐的药物诱导毒性以及住院时间延长。据报道,在氟康唑基础上加用单次高剂量的脂质体两性霉素(L-AmB,安必素)在减轻真菌负荷方面不劣于14天标准剂量的L-AmB。本试验旨在研究高剂量氟康唑和氟胞嘧啶联用单次高剂量L-AmB是否不劣于为期七天的两性霉素B脱氧胆酸盐加氟胞嘧啶疗程(世界卫生组织[WHO]目前推荐的治疗方案)。
在撒哈拉以南非洲的五个国家(博茨瓦纳、马拉维、南非、乌干达和津巴布韦)开展一项开放标签的III期随机对照非劣效性试验。该试验将比较CM诱导疗法,即(1)单次剂量(10mg/kg)的L-AmB联用14天的氟康唑(1200mg/天)和氟胞嘧啶(100mg/kg/天)与(2)七天的两性霉素B脱氧胆酸盐(1mg/kg/天)加七天的氟胞嘧啶(100mg/kg/天),随后七天使用氟康唑(1200mg/天)。主要终点是十周时的全因死亡率,非劣效性界值为10%,检验效能为90%。次要终点包括早期杀菌活性、III/IV级不良事件的比例、药代动力学参数和药代动力学/药效学关联、卫生服务成本、前两周和四周内的全因死亡率、前十周内的全因死亡率(优效性分析)以及十周时CM复发率、免疫重建炎症综合征和残疾率。总共将招募850名年龄≥18岁的HIV相关CM首发患者(每组随机分配425名)。所有患者将接受16周的随访。所有患者将接受氟康唑800mg/天的巩固治疗以完成十周的治疗,随后根据当地指南进行氟康唑维持治疗和ART。
一种安全、可持续且易于给药的L-AmB方案,若不劣于为期七天的每日两性霉素B脱氧胆酸盐治疗,可能会减少接受两性霉素B脱氧胆酸盐治疗患者出现的不良事件数量,并缩短住院时间,为当前WHO推荐的一线治疗提供一种非常有利且可实施的替代方案。
ISRCTN,ISRCTN:72509687。于2017年7月13日注册。