Department of Public Health and Primary Care, University of Cambridge, 2 Worts' Causeway, Cambridge, UK.
Department of Physiology, Development and Neuroscience, University of Cambridge, Downing Street, Cambridge, UK.
Eur Heart J. 2019 Feb 14;40(7):621-631. doi: 10.1093/eurheartj/ehy653.
There is debate about the optimum algorithm for cardiovascular disease (CVD) risk estimation. We conducted head-to-head comparisons of four algorithms recommended by primary prevention guidelines, before and after 'recalibration', a method that adapts risk algorithms to take account of differences in the risk characteristics of the populations being studied.
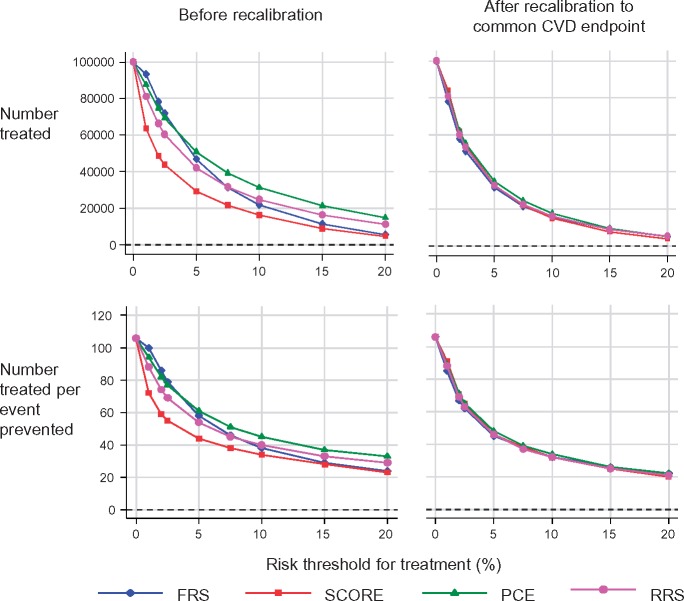
Using individual-participant data on 360 737 participants without CVD at baseline in 86 prospective studies from 22 countries, we compared the Framingham risk score (FRS), Systematic COronary Risk Evaluation (SCORE), pooled cohort equations (PCE), and Reynolds risk score (RRS). We calculated measures of risk discrimination and calibration, and modelled clinical implications of initiating statin therapy in people judged to be at 'high' 10 year CVD risk. Original risk algorithms were recalibrated using the risk factor profile and CVD incidence of target populations. The four algorithms had similar risk discrimination. Before recalibration, FRS, SCORE, and PCE over-predicted CVD risk on average by 10%, 52%, and 41%, respectively, whereas RRS under-predicted by 10%. Original versions of algorithms classified 29-39% of individuals aged ≥40 years as high risk. By contrast, recalibration reduced this proportion to 22-24% for every algorithm. We estimated that to prevent one CVD event, it would be necessary to initiate statin therapy in 44-51 such individuals using original algorithms, in contrast to 37-39 individuals with recalibrated algorithms.
Before recalibration, the clinical performance of four widely used CVD risk algorithms varied substantially. By contrast, simple recalibration nearly equalized their performance and improved modelled targeting of preventive action to clinical need.
关于心血管疾病(CVD)风险评估的最佳算法存在争议。我们在“重新校准”前后,对四项推荐的一级预防指南算法进行了头对头比较,“重新校准”是一种使风险算法适应所研究人群风险特征差异的方法。
利用来自 22 个国家 86 项前瞻性研究的 360737 例无 CVD 的基线参与者的个体参与者数据,我们比较了Framingham 风险评分(FRS)、系统性冠状动脉风险评估(SCORE)、汇总队列方程(PCE)和 Reynolds 风险评分(RRS)。我们计算了风险区分度和校准度的指标,并对判断为 10 年 CVD 风险“高”的人群启动他汀类药物治疗的临床意义进行了建模。原始风险算法使用目标人群的风险因素特征和 CVD 发生率进行了重新校准。在重新校准之前,FRS、SCORE 和 PCE 平均高估 CVD 风险 10%、52%和 41%,而 RRS 低估 10%。原始算法将 29-39%的≥40 岁人群分类为高危人群。相比之下,每个算法的重新校准版本将这一比例降低到 22-24%。我们估计,使用原始算法,需要在 44-51 名此类个体中启动他汀类药物治疗,才能预防 1 例 CVD 事件,而在使用重新校准算法时,只需在 37-39 名个体中启动他汀类药物治疗。
在重新校准之前,四种广泛使用的 CVD 风险算法的临床性能差异很大。相比之下,简单的重新校准几乎可以使它们的性能均等化,并改善了对预防措施的建模靶向以满足临床需求。