Kil Hae Keum, Kim Ji Young, Choi Young Deuk, Lee Hye Sun, Kim Tae Kwang, Kim Ji Eun
Department of Anesthesiology and Pain Medicine, Anesthesia and Pain Research Institute, Yonsei University College of Medicine, Seoul 03722, Korea.
Department of Urology, Yonsei University College of Medicine, Seoul 03722, Korea.
J Clin Med. 2018 Nov 23;7(12):470. doi: 10.3390/jcm7120470.
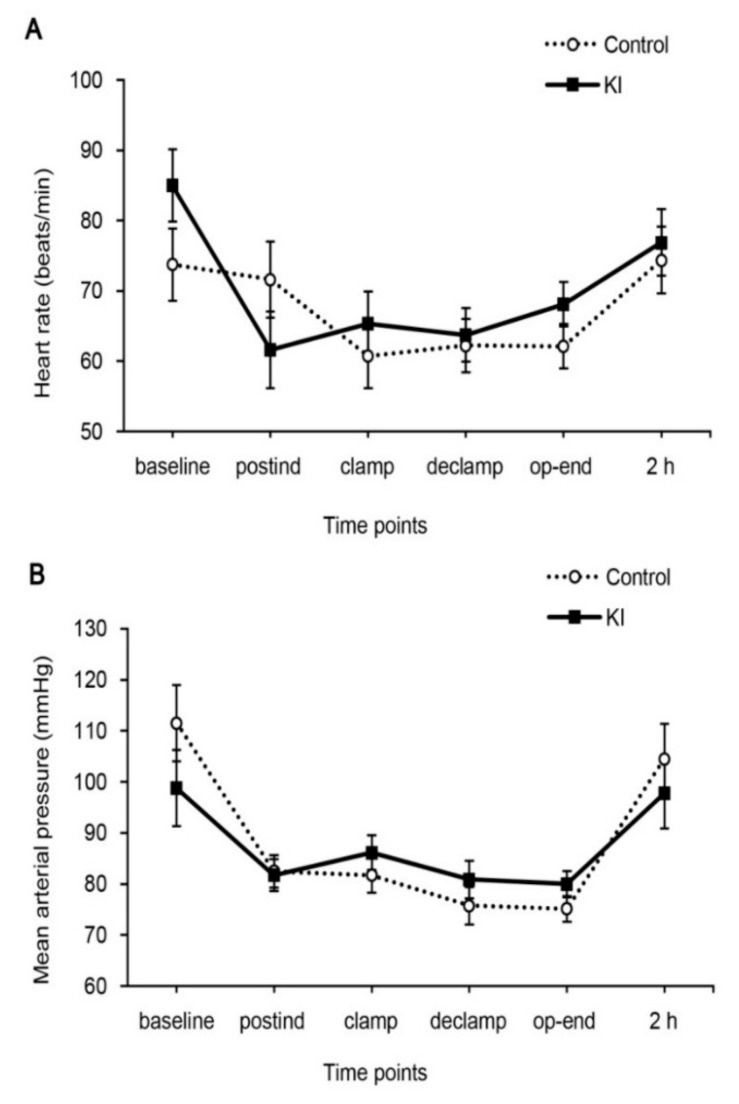
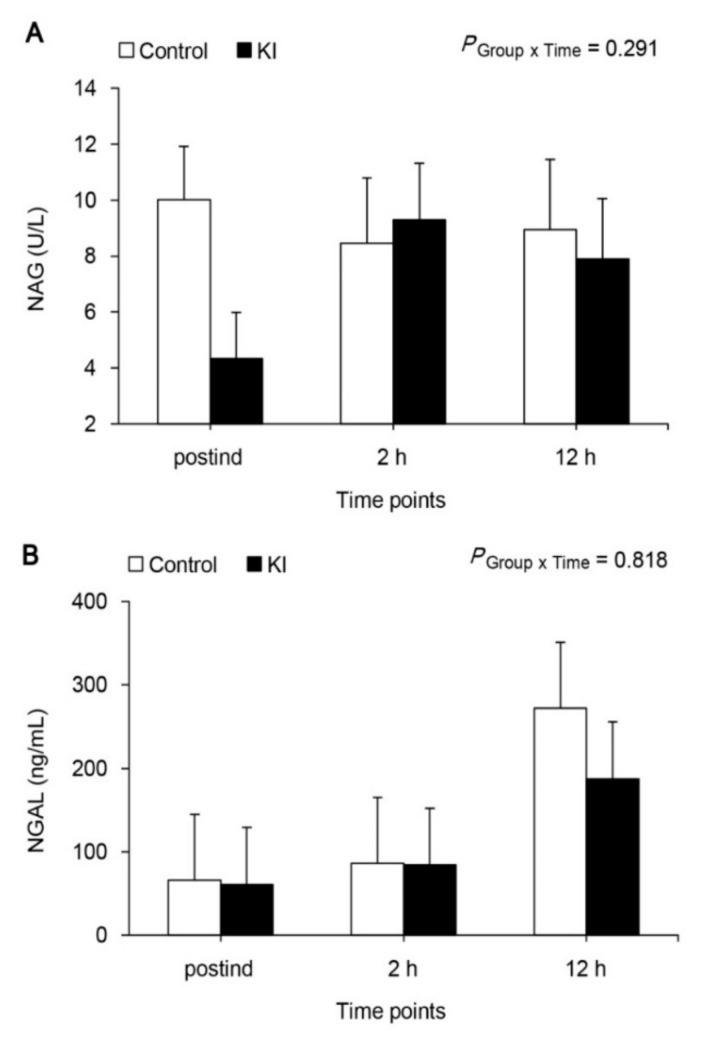
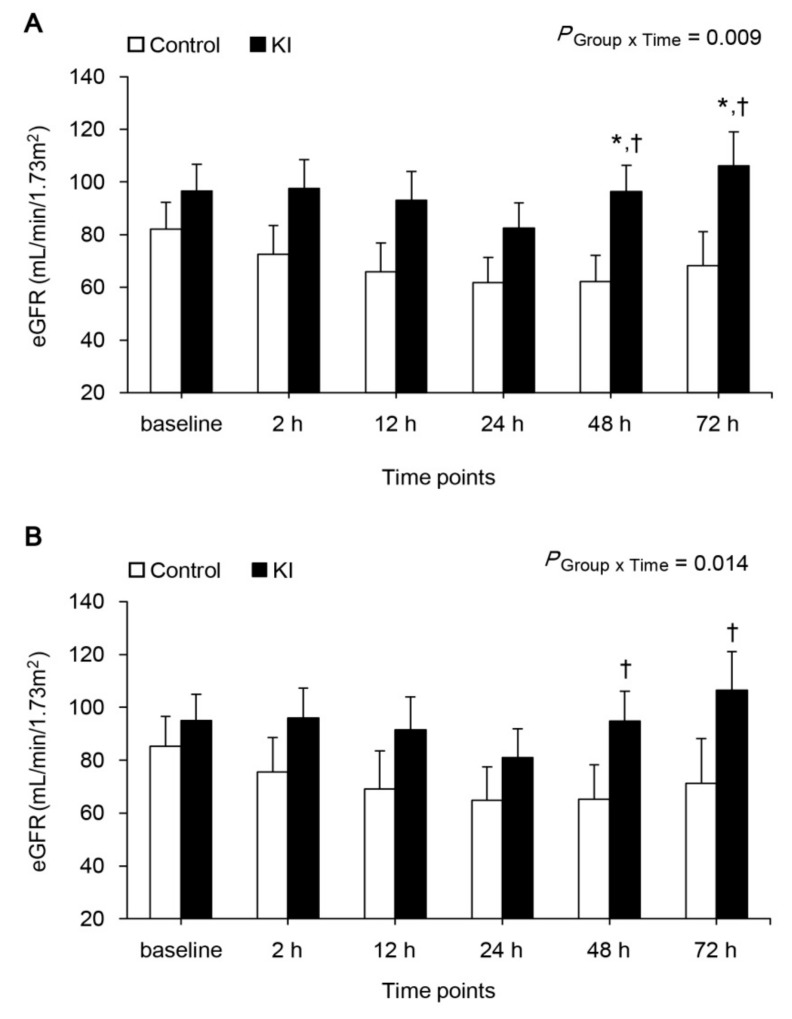
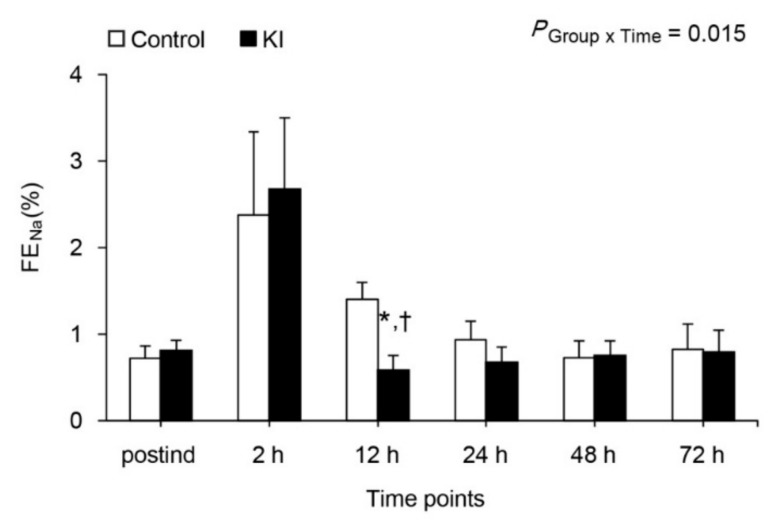
We evaluated postoperative renal function in patients with/without combined therapy of ketorolac and remote ischemic preconditioning during partial nephrectomy. Sixteen patients were randomly allocated to either the ketorolac combined with RIPC group (KI, = 8) or control group ( = 8). The KI group received both remote ischemic preconditioning before surgery and intravenous ketorolac of 1 mg/kg before renal artery clamping. Renal parameters were measured before induction, after anesthesia induction, and 2, 12, 24, 48, and 72 h after renal artery declamping. Acute kidney injury was assessed by Acute Kidney Injury Network criteria. The estimated glomerular filtration rate decreased in both groups, but then increased significantly at 48 h and 72 h after declamping only in the KI group compared to 24 h ( = 0.001 and = 0.016). Additionally, it was higher at 48 h and 72 h after declamping in the KI group compared to the control group ( = 0.025 and = 0.044). The incidence of acute kidney injury was significantly reduced in the KI group (13%) compared to the control group (83%) ( = 0.026). FE was markedly increased at 2 h after declamping, and recovered in both groups, but it was more significant at 12 h after declamping in the KI group ( = 0.022). Urinary N-acetyl-1-β-D-glucosoaminidase and serum neutrophil gelatinase-associated lipocalin were similar ( = 0.291 and = 0.818). There is a possibility that combined therapy of ketorolac and remote ischemic preconditioning prior to ischemia may alleviate renal dysfunction and reduce the incidence of acute kidney injury in patients undergoing partial nephrectomy.
我们评估了在部分肾切除术期间接受/未接受酮咯酸与远程缺血预处理联合治疗的患者的术后肾功能。16例患者被随机分配至酮咯酸联合远程缺血预处理组(KI组,n = 8)或对照组(n = 8)。KI组在手术前接受远程缺血预处理,并在肾动脉夹闭前静脉注射1mg/kg酮咯酸。在诱导前、麻醉诱导后以及肾动脉松开后2、12、24、48和72小时测量肾脏参数。根据急性肾损伤网络标准评估急性肾损伤。两组的估计肾小球滤过率均下降,但与24小时相比,仅KI组在松开后48小时和72小时显著升高(P = 0.001和P = 0.016)。此外,与对照组相比,KI组在松开后48小时和72小时时更高(P = 0.025和P = 0.044)。与对照组(83%)相比,KI组急性肾损伤的发生率显著降低(13%)(P = 0.026)。FE在松开后2小时显著升高,两组均恢复,但KI组在松开后12小时更为显著(P = 0.022)。尿N-乙酰-β-D-氨基葡萄糖苷酶和血清中性粒细胞明胶酶相关脂质运载蛋白相似(P = 0.291和P = 0.818)。酮咯酸与缺血前远程缺血预处理联合治疗有可能减轻接受部分肾切除术患者的肾功能障碍并降低急性肾损伤的发生率。