Visser Janicke, McLachlan Milla H, Maayan Nicola, Garner Paul
Division of Human Nutrition, Stellenbosch University, Francie van Zijl Drive, Cape Town, Western Cape, South Africa, 7505.
Cochrane Database Syst Rev. 2018 Nov 9;11(11):CD010578. doi: 10.1002/14651858.CD010578.pub2.
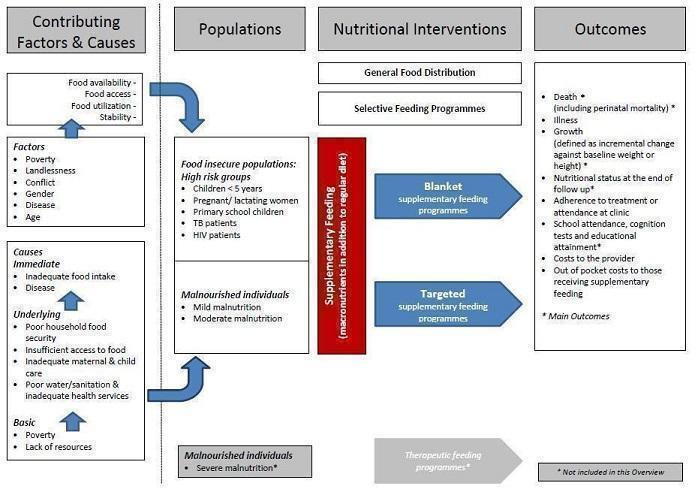
Supplementary feeding may help food insecure and vulnerable people by optimising the nutritional value and adequacy of the diet, improving quality of life and improving various health parameters of disadvantaged families. In low- and middle-income countries (LMIC), the problems supplementary feeding aims to address are entangled with poverty and deprivation, the programmes are expensive and delivery is complicated.
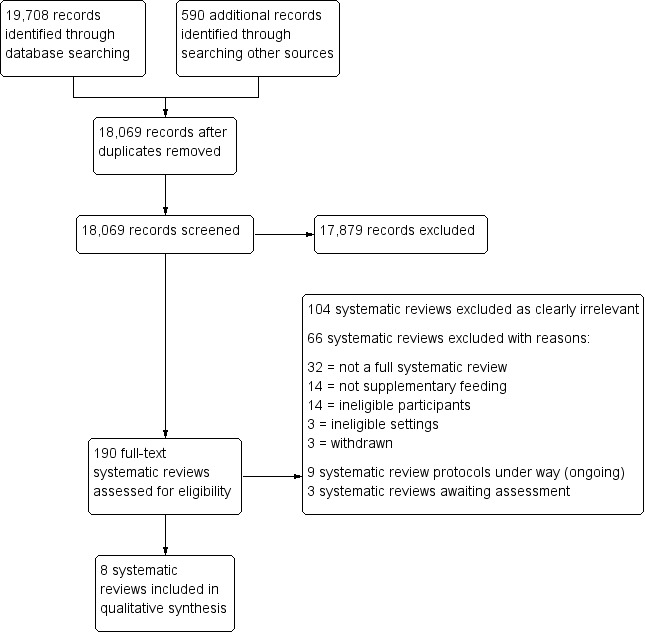
In January 2017, we searched the Cochrane Database of Systematic Reviews, MEDLINE, Embase and nine other databases. We included systematic reviews evaluating community-based supplementary feeding, and concerning food insecure, vulnerable and malnourished populations. Two review authors independently undertook selection of systematic reviews, data extraction and 'Risk of bias' assessment. We assessed review quality using the AMSTAR tool, and used GRADEpro 'Summary of findings' tables from each review to indicate the certainty of the evidence for the main comparisons. We summarised review findings in the text and reported the data for each outcome in additional tables. We also used forest plots to display results graphically.
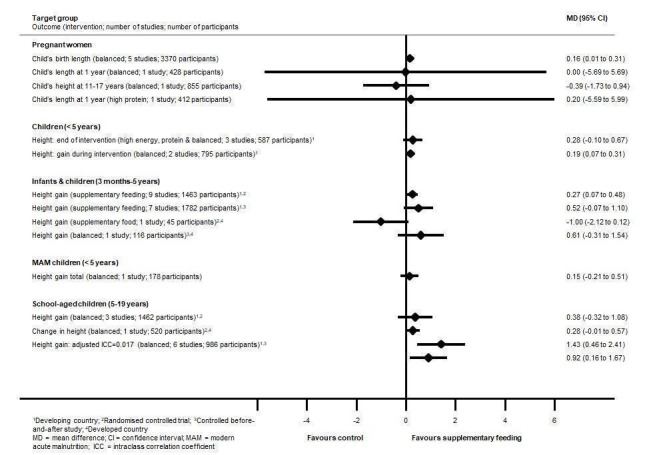
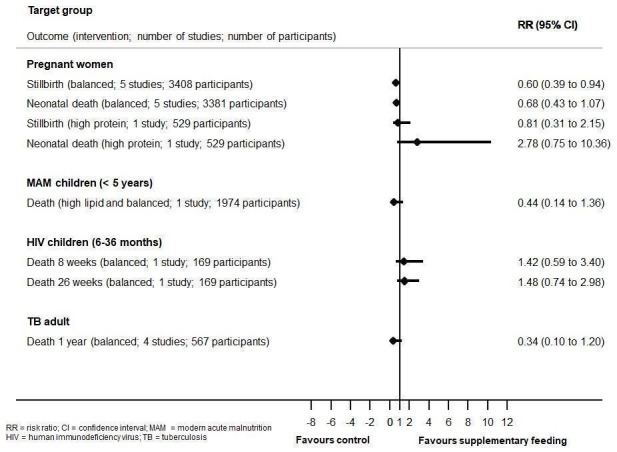
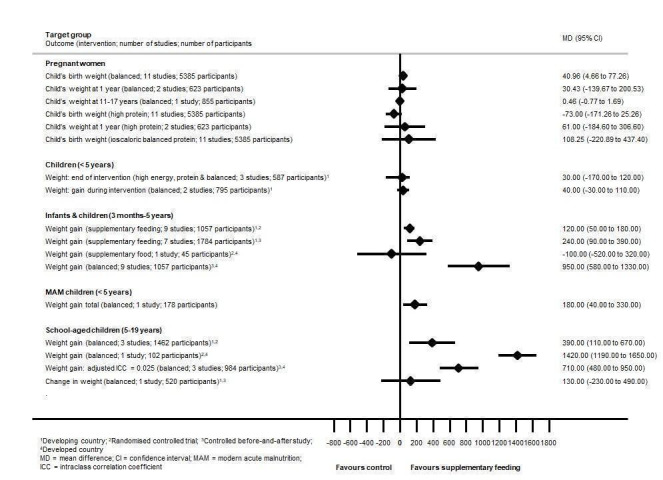
This overview included eight systematic reviews (with last search dates between May 2006 and February 2016). Seven were Cochrane Reviews evaluating interventions in pregnant women; children (aged from birth to five years) from LMIC; disadvantaged infants and young children (aged three months to five years); children with moderate acute malnutrition (MAM); disadvantaged school children; adults and children who were HIV positive or with active tuberculosis (with or without HIV). One was a non-Cochrane systematic review in older people with Alzheimer's disease. These reviews included 95 trials relevant to this overview, with the majority (74%) of participants from LMIC.The number of included participants varied between 91 and 7940 adults, and 271 and more than 12,595 children. Trials included a wide array of nutritional interventions that varied in duration, frequency and format, with micronutrients often reported as cointerventions. Follow-up ranged from six weeks to two years; three trials investigated outcomes at four to 17 years of age. All reviews were rated as high quality (AMSTAR score between eight and 11). The GRADE certainty ratings ranged from very low to moderate for individual comparisons, with the evidence often comprising only one or two small trials, thereby resulting in many underpowered analyses (too small to detect small but important differences). The main outcome categories reported across reviews were death, anthropometry (adults and children) and other markers of nutritional status, disease-related outcomes, neurocognitive development and psychosocial outcomes, and adverse events.Mortality data were limited and underpowered in meta-analysis in all populations (children with MAM, in children with HIV, and in adults with tuberculosis) with the exception of balanced energy and protein supplementation in pregnancy, which may have reduced the risk of stillbirth (risk ratio (RR) 0.60, 95% confidence interval (CI) 0.39 to 0.94; 5 trials, 3408 women). Supplementation in pregnancy also improved infant birth weight (mean difference (MD) 40.96 g, 95% CI 4.66 to 77.26; 11 trials, 5385 participants) and reduced risk of infants born small-for-gestational age (RR 0.79, 95% CI 0.69 to 0.90; 7 trials, 4408 participants). These effects did not translate into demonstrable long-term benefits for children in terms of growth and neurocognitive development in the one to two trials reporting on longer-term outcomes. In one study (505 participants), high-protein supplementation was associated with increased risk of small-for-gestational age babies.Effects on growth in children were mixed. In children under five years of age from LMIC, one review found that supplementary feeding had a little or no effect on child growth; however, a more recent review in a similar population found that those who received food supplementation gained an average of 0.12 kg more in weight (MD 0.12 kg, 95% CI 0.05 to 0.18; 9 trials, 1057 participants) and 0.27 cm more in height (MD 0.27 cm, 95% CI 0.07 to 0.48; 9 trials, 1463 participants) than those who were not supplemented. Supplementary food was generally more effective for younger children (younger than two years of age) and for those who were poorer or less well-nourished. In children with MAM, the provision of specially formulated food improved their weight, weight-for-height z scores and other key outcomes such as recovery rate (by 29%), as well as reducing the number of participants dropping out (by 70%). In LMIC, school meals seemed to lead to small benefits for children, including improvements in weight z scores, especially in children from lower-income countries, height z scores, cognition or intelligence quotient tests, and maths and spelling performance.Supplementary feeding in adults who were HIV positive increased the daily energy and protein intake compared to nutritional counselling alone. Supplementation led to an initial improvement in weight gain or body mass index but did not seem to confer long-term benefit.In adults with tuberculosis, one small trial found a significant benefit on treatment completion and sputum conversion rate. There were also significant but modest benefits in terms of weight gain (up to 2.60 kg) during active tuberculosis.The one study included in the Alzheimer's disease review found that three months of daily oral nutritional supplements improved nutritional outcomes in the intervention group.There was little or no evidence regarding people's quality of life, adherence to treatment, attendance at clinic or the costs of supplementary feeding programmes.
AUTHORS' CONCLUSIONS: Considering the current evidence base included, supplementary food effects are modest at best, with inconsistent and limited mortality evidence. The trials reflected in the reviews mostly reported on short-term outcomes and across the whole of the supplementation trial literature it appears important outcomes, such as quality of life and cost of programmes, are not systematically reported or summarised.
补充喂养可通过优化饮食的营养价值和充足性、改善生活质量以及改善弱势家庭的各项健康指标,帮助粮食不安全和脆弱人群。在低收入和中等收入国家(LMIC),补充喂养旨在解决的问题与贫困和匮乏交织在一起,这些项目成本高昂且实施复杂。
2017年1月,我们检索了Cochrane系统评价数据库、MEDLINE、Embase和其他九个数据库。我们纳入了评估基于社区的补充喂养以及涉及粮食不安全、脆弱和营养不良人群的系统评价。两位评价作者独立进行系统评价的选择、数据提取和“偏倚风险”评估。我们使用AMSTAR工具评估评价质量,并使用每个评价的GRADEpro“结果总结”表来表明主要比较证据的确定性。我们在正文中总结评价结果,并在附加表格中报告每个结果的数据。我们还使用森林图以图形方式展示结果。
本概述纳入了八项系统评价(最后检索日期在2006年5月至2016年2月之间)。七项是Cochrane评价,评估了对孕妇;来自低收入和中等收入国家的儿童(从出生到五岁);弱势婴幼儿(三个月至五岁);中度急性营养不良(MAM)儿童;弱势学龄儿童;艾滋病毒呈阳性或患有活动性结核病的成人和儿童(有无艾滋病毒)的干预措施。一项是非Cochrane系统评价,针对患有阿尔茨海默病的老年人。这些评价纳入了95项与本概述相关的试验,其中大多数(74%)参与者来自低收入和中等收入国家。纳入的参与者数量在91至7940名成人以及271至超过12595名儿童之间。试验包括一系列营养干预措施,其持续时间、频率和形式各不相同,微量营养素通常作为联合干预措施报告。随访时间从六周至两年;三项试验在4至17岁时调查结果。所有评价均被评为高质量(AMSTAR评分在8至11之间)。对于个体比较,GRADE确定性评级从极低到中等不等,证据通常仅包括一两项小型试验,因此导致许多分析效能不足(样本量太小,无法检测到虽小但重要的差异)。各评价报告的主要结果类别包括死亡、人体测量(成人和儿童)以及营养状况的其他指标、疾病相关结果、神经认知发育和心理社会结果以及不良事件。除了孕期补充均衡能量和蛋白质可能降低死产风险(风险比(RR)0.60,95%置信区间(CI)0.39至0.94;5项试验,3408名女性)外,所有人群(MAM儿童、艾滋病毒感染儿童和结核病成人)的死亡率数据在荟萃分析中都很有限且效能不足。孕期补充营养还改善了婴儿出生体重(平均差(MD)40.96克,95%CI 4.66至77.26;11项试验,5385名参与者),并降低了小于胎龄儿出生风险(RR 0.79,9