Niederseer David, Bracher Isabelle, Stadlmayr Andreas, Huber-Schönauer Ursula, Plöderl Martin, Obeid Slayman, Schmied Christian, Hammerl Sabrina, Stickel Felix, Lederer Dieter, Patsch Wolfgang, Aigner Elmar, Datz Christian
Department of Internal Medicine, General Hospital Oberndorf, Teaching Hospital of the Paracelsus Medical University Salzburg, 5110 Oberndorf, Austria.
Department of Cardiology, University Heart Centre, University Hospital Zurich, 8091 Zürich, Switzerland.
J Clin Med. 2018 Nov 27;7(12):484. doi: 10.3390/jcm7120484.
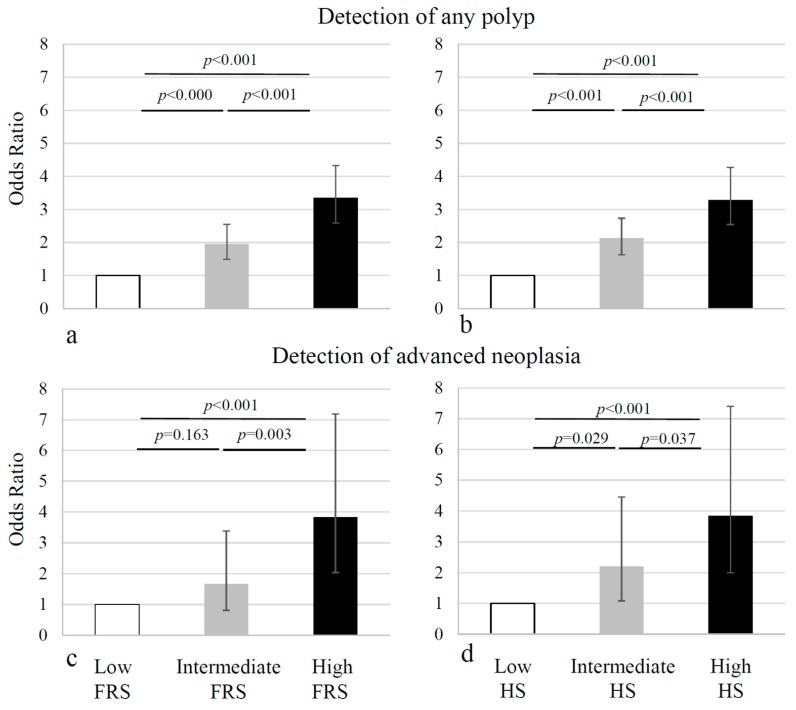
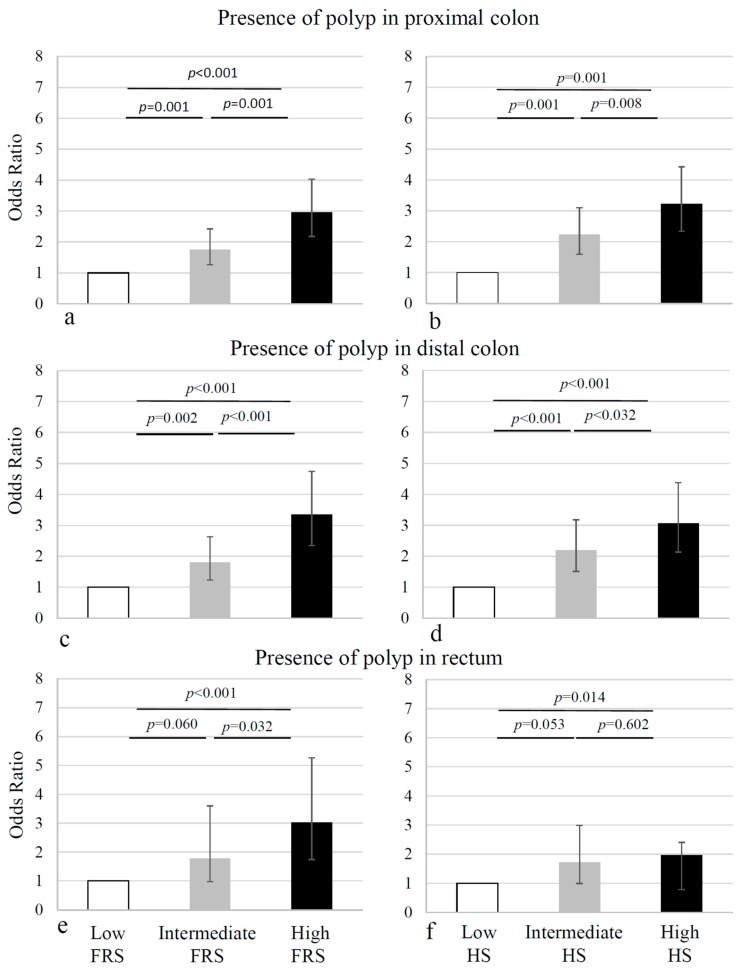
Several studies have shown site-specific differences in colorectal cancer (CRC) with respect to the risk factors. CRC was shown to be associated with cardiovascular risk (CVR) factors, but site-specific variations have not been investigated so far. This study aimed to assess the associations between the prevalence and subsite-specific differences of colorectal neoplasia and established CVR scores or known coronary artery disease (CAD) in a large asymptomatic European screening cohort ( = 2098). Participants underwent simultaneous screening colonoscopy and CVR evaluation, using the Framingham Risk Score and Heart Score. Lesions found in the colonoscopy were classified by location (proximal/distal colon or rectum). More neoplasias were found in the proximal versus the distal colon ( < 0.001). The Framingham Risk Score and Heart Score showed incremental risk for colorectal adenoma, across the tertiles in the proximal and the distal colon ( < 0.001). The prevalence of adenomas in the rectum was much lower, but also here, incremental risk could be shown for the Framingham Risk but not the Heart Risk Score tertiles. Prevalence of adenomas in the proximal colon was higher in subjects with type 2 diabetes (T2DM) ( = 0.006), but no association was found between adenomas and T2DM in the distal colon ( = 0.618) and the rectum ( = 0.071). Males had a higher CVR and more findings, in the screening colonoscopy, as compared to females, however, no site-specific differences were noted. Patients with known CAD and high CVR have an increased risk of colorectal neoplasia in both the proximal and distal colon. Patients with T2DM have a higher risk for neoplasia in the proximal colon.
多项研究表明,结直肠癌(CRC)在风险因素方面存在部位特异性差异。CRC已被证明与心血管风险(CVR)因素相关,但迄今为止尚未对部位特异性差异进行研究。本研究旨在评估在一个大型无症状欧洲筛查队列(n = 2098)中,结直肠肿瘤的患病率和部位特异性差异与既定的CVR评分或已知冠状动脉疾病(CAD)之间的关联。参与者同时接受结肠镜检查和CVR评估,使用弗雷明汉风险评分和心脏评分。结肠镜检查中发现的病变按位置(近端/远端结肠或直肠)分类。近端结肠发现的肿瘤比远端结肠更多(P < 0.001)。弗雷明汉风险评分和心脏评分显示,在近端和远端结肠的三分位数中,结直肠腺瘤的风险呈递增趋势(P < 0.001)。直肠腺瘤的患病率低得多,但在这里,弗雷明汉风险评分三分位数也显示出递增风险,而心脏风险评分三分位数则未显示。2型糖尿病(T2DM)患者近端结肠腺瘤的患病率较高(P = 0.006),但在远端结肠(P = 0.618)和直肠(P = 0.071)中未发现腺瘤与T2DM之间存在关联。与女性相比,男性的CVR更高,在筛查结肠镜检查中发现的病变更多,然而,未观察到部位特异性差异。已知患有CAD和高CVR的患者在近端和远端结肠患结直肠肿瘤的风险均增加。T2DM患者近端结肠患肿瘤的风险更高。