Clinical Research Center for Rare Diseases Aldo e Cele Daccò and Centro Anna Maria Astori, Science and Technology Park Kilometro Rosso, Istituto di Ricerche Farmacologiche Mario Negri IRCCS, Bergamo, Italy.
Unit of Nephrology and Dialysis, Azienda Socio-Sanitaria Territoriale Papa Giovanni XXIII, Bergamo, Italy.
Front Immunol. 2018 Oct 15;9:2329. doi: 10.3389/fimmu.2018.02329. eCollection 2018.
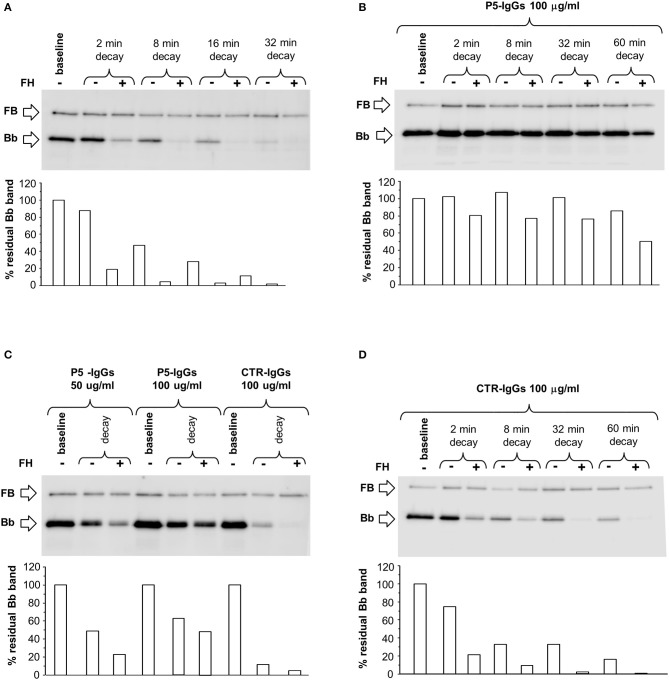
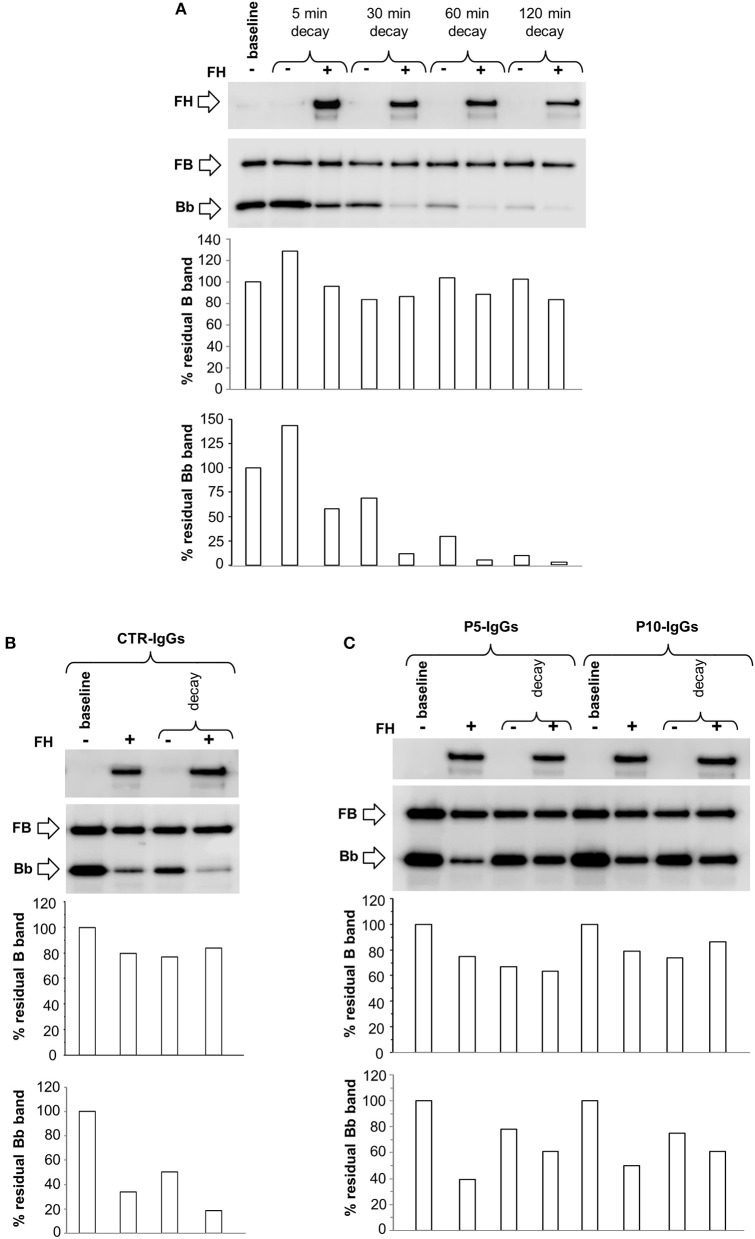
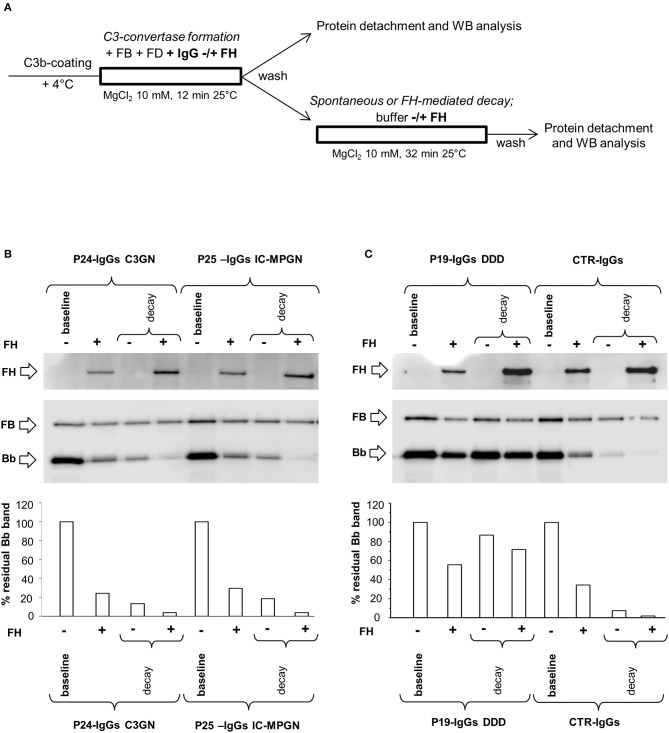
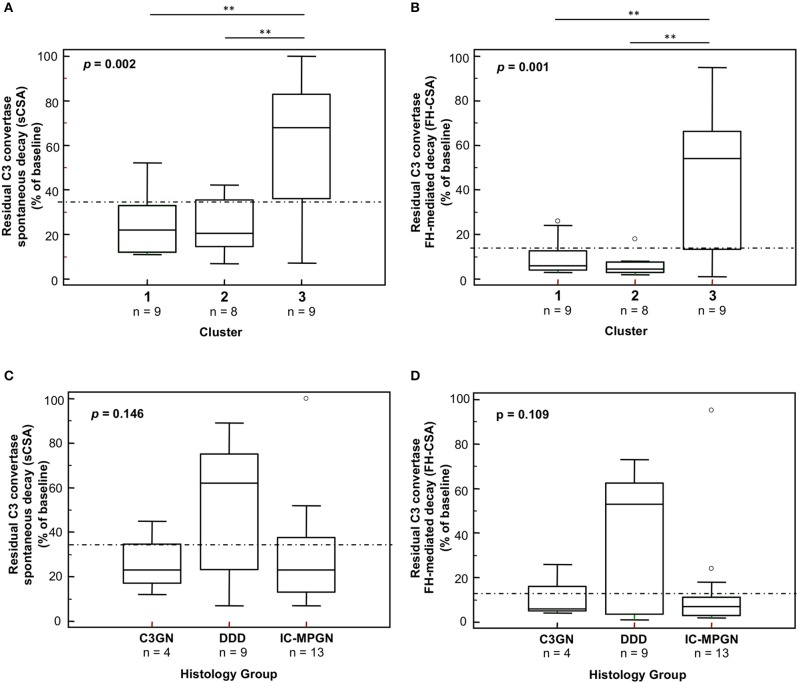
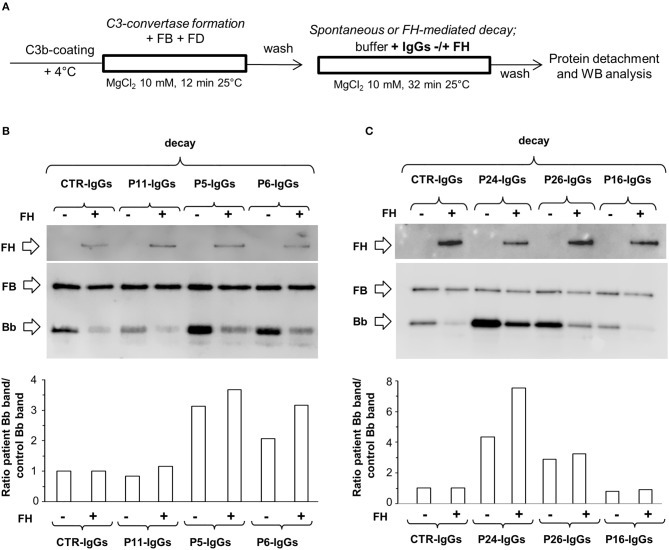
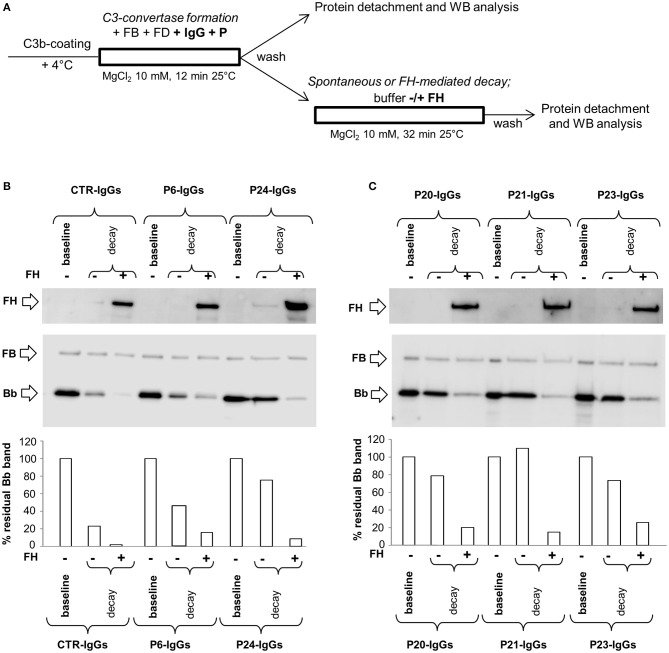
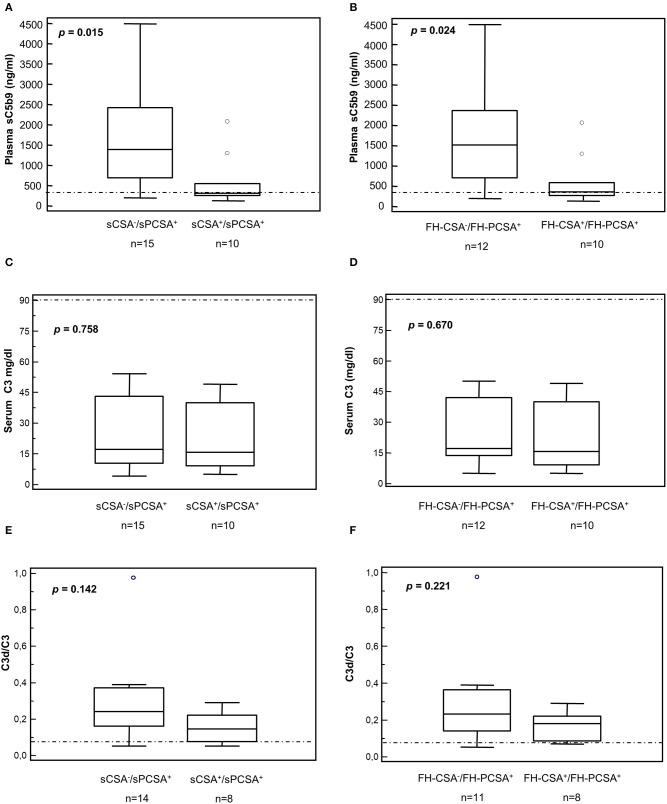
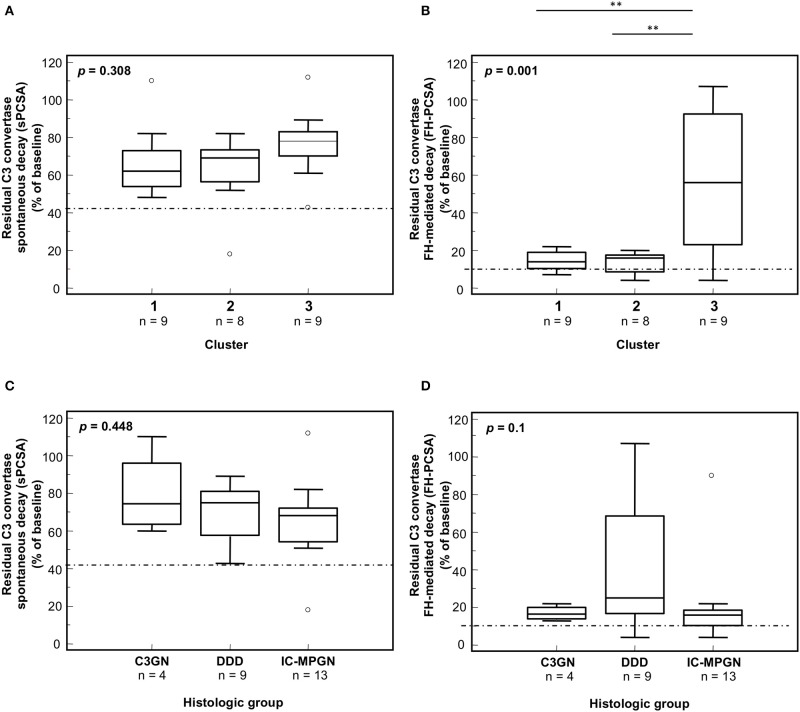
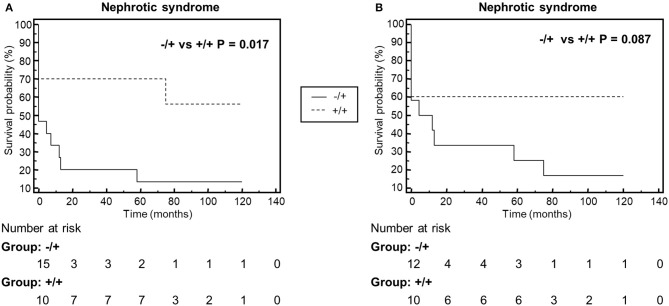
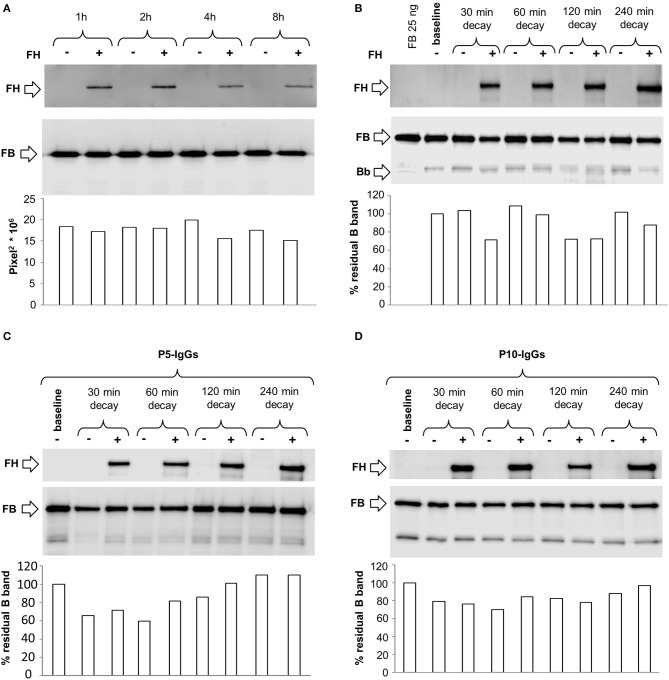
Membranoproliferative glomerulonephritis (MPGN) was recently classified as C3 glomerulopathies (C3G), and immune-complex (IC) mediated MPGN. Dysregulation of the complement alternative pathway, driven by acquired and/or genetic defects, plays a pathogenetic role in C3G. However, alternative pathway abnormalities were also found in IC-MPGN. The most common acquired drivers are the C3 nephritic factors (C3NeFs), heterogeneous autoantibodies that stabilize the C3 convertase, C3bBb. C3NeFs are traditionally detected by hemolytic assays based on sheep erythrocyte lysis, which however do not provide a direct molecular estimation of C3bBb formation and decay. We set up a microplate/western blot assay that specifically detects and quantifies C3bBb, and its precursor, the C3 proconvertase C3bB, to investigate the complex mechanistic effects of C3NeFs from patients with primary IC-MPGN ( = 13) and C3G ( = 13). In the absence of properdin, 9/26 patients had C3NeF IgGs stabilizing C3bBb against spontaneous and FH-accelerated decay. In the presence of properdin the IgGs of all but one patient had C3bBb-stabilizing activity. Properdin-independent C3NeFs were identified mostly in DDD patients, while properdin-dependent C3NeFs associated with either C3GN or IC-MPGN and with higher incidence of nephrotic syndrome. When we grouped patients based on our recent cluster analysis, patients in cluster 3, with highly electron-dense intramembranous deposits, low C3, and mostly normal sC5b-9 levels, had a higher prevalence of properdin-independent C3NeFs than patients in clusters 1 and 2. Conversely, about 70% of cluster 1 and 2 patients, with subendothelial, subepithelial, and mesangial deposits, low C3 levels and high sC5b-9 levels, had properdin-dependent C3NeFs. The flexibility of the assay allowed us to get deep insights into C3NeF mechanisms of action, showing that: (1) most C3NeFs bind strongly and irreversibly to C3 convertase; (2) C3NeFs and FH recognize different epitopes in C3 convertase; (3) C3NeFs bind rapidly to C3 convertase and antagonize the decay accelerating activity of FH on newly formed complexes; (4) C3NeFs do not affect formation and stability of the C3 proconvertase. Thus, our study provides a molecular approach to detecting and characterizing C3NeFs. The results highlight different mechanisms of complement dysregulation resulting in different complement profiles and patterns of glomerular injury, and this may have therapeutic implications.
补体替代途径的失调,由获得性和/或遗传性缺陷驱动,在 C3 肾小球疾病(C3G)中发挥致病作用。然而,免疫复合物(IC)介导的 MPGN 也存在补体替代途径异常。最常见的获得性驱动因素是 C3 肾炎因子(C3NeFs),这是一种稳定 C3 转化酶 C3bBb 的异质性自身抗体。C3NeFs 传统上通过基于绵羊红细胞裂解的溶血测定法检测,但不能直接对 C3bBb 的形成和降解进行分子估计。我们建立了一种微孔板/免疫印迹测定法,该方法专门检测和定量 C3bBb 及其前体 C3 原转化酶 C3bB,以研究来自原发性 IC-MPGN(n = 13)和 C3G(n = 13)患者的 C3NeFs 的复杂机制作用。在没有备解素的情况下,9/26 名患者的 C3NeF IgG 稳定了 C3bBb,使其免受自发和 FH 加速的衰变。在备解素存在的情况下,除了一名患者外,所有患者的 IgG 均具有 C3bBb 稳定活性。大多数 DDD 患者存在备解素非依赖性 C3NeFs,而备解素依赖性 C3NeFs 与 C3GN 或 IC-MPGN 相关,且肾病综合征的发病率更高。当我们根据最近的聚类分析对患者进行分组时,在簇 3 中,具有高度电子致密的内皮下沉积物、C3 水平较低且 sC5b-9 水平大多正常的患者比簇 1 和 2 中的患者更易出现备解素非依赖性 C3NeFs。相反,簇 1 和 2 中约 70%的患者具有内皮下、上皮下和系膜沉积物、C3 水平低和 sC5b-9 水平高的患者具有备解素依赖性 C3NeFs。该测定法的灵活性使我们能够深入了解 C3NeF 的作用机制,表明:(1)大多数 C3NeF 与 C3 转化酶结合牢固且不可逆;(2)C3NeF 和 FH 在 C3 转化酶上识别不同的表位;(3)C3NeF 快速结合 C3 转化酶,并拮抗 FH 对新形成复合物的衰变加速活性;(4)C3NeF 不影响 C3 原转化酶的形成和稳定性。因此,我们的研究提供了一种检测和表征 C3NeF 的分子方法。结果突出了补体失调导致不同补体谱和肾小球损伤模式的不同机制,这可能具有治疗意义。