Department of Cardiac Surgery, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of Medicine, Tel Aviv University, 52621, Tel Aviv, Israel.
Cardiac Surgery Intensive Care Unit, Sheba Medical Center, Tel Hashomer, Affiliated to the Sackler School of Medicine, Tel Aviv University, Tel Aviv, Israel.
Cardiovasc Diabetol. 2018 Nov 29;17(1):151. doi: 10.1186/s12933-018-0796-7.
Type 2 diabetes mellitus (DM) is a frequent co-morbidity among patients undergoing coronary artery bypass grafting (CABG) surgery. The aim of this study was to evaluate the impact of DM on the early- and long-term outcomes of patients who underwent isolated CABG.
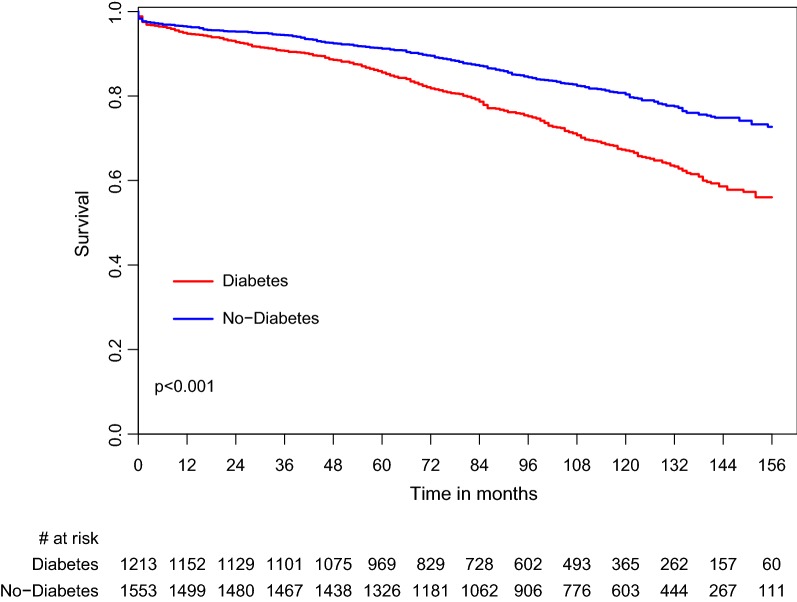
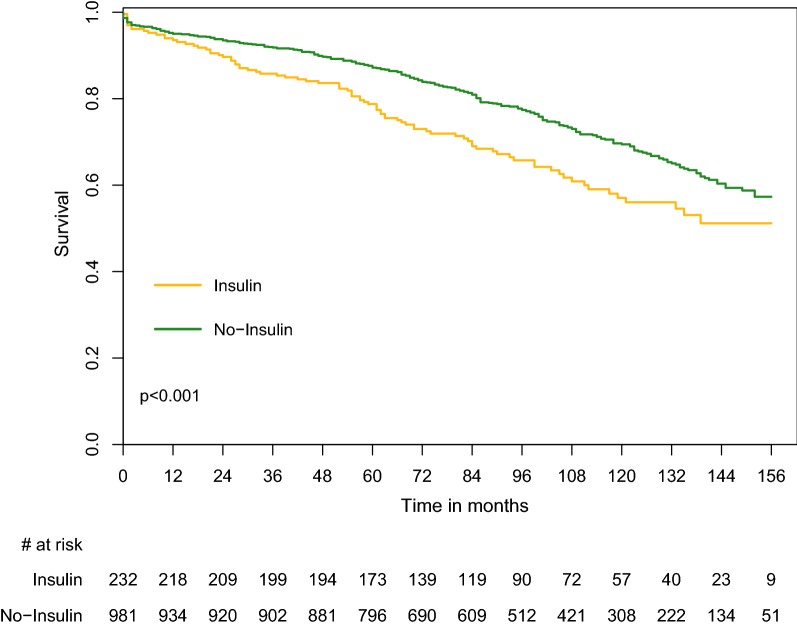
We performed an observational cohort study in a large tertiary medical center over a period of 11 years. All data from patients who had undergone isolated CABG surgery between 2004 and 2014 were obtained from our departmental database. The study population included 2766 patients who were divided into two groups: Group I (1553 non-diabetic patients), and Group II (1213 patients suffering from type 2 DM). Group II patients were then divided into two subgroups: subgroup IIA (981 patients treated with oral antihyperglycemic medications) and subgroup IIB (232 insulin-treated patients with or without additional oral antihyperglycemic drugs). In-hospital, 1-, 3-, 5- and 10-year mortality outcome variables were evaluated. Mean follow-up was 97 ± 41 months.
In-hospital mortality was similar between Group I and Group II patients (1.87% vs. 2.31%, p = 0.422) and between the subgroups IIA and IIB (2.14% vs. 3.02%, p = 0.464). Long-term mortality (1, 3, 5 and 10 years) was higher in Group II (DM type 2) compared with Group I (non-diabetic patients) (5.3% vs. 3.6%, p = 0.038; 9.3% vs. 5.6%, p < 0.001; 15.3% vs. 9.3%, p < 0.001 and 47.3% vs. 29.6% p < 0.001). Kaplan-Meier analysis demonstrated that all-cause mortality was higher in Group II compared with Group I (p < 0.001) and in subgroup IIB compared with subgroup IIA (p = 0.001). Multivariable analysis showed that DM increased the mortality hazard by twofold, and among diabetic patients, insulin treatment increased the mortality hazard by twofold.
Diabetic and non-diabetic patients have similar in-hospital mortality rates. Survival rates of diabetic patients start to deteriorate 3 year after surgery. Type 2 DM is an independent predictor for long-term mortality after isolated CABG surgery. Mortality is even higher when the diabetes treatment strategy included insulin.
2 型糖尿病(DM)是接受冠状动脉旁路移植术(CABG)的患者常见的合并症。本研究的目的是评估 DM 对接受单纯 CABG 患者的早期和长期结局的影响。
我们在一个大型三级医疗中心进行了一项观察性队列研究,时间跨度为 11 年。从我们科室数据库中获取了 2004 年至 2014 年间接受单纯 CABG 手术的所有患者的数据。研究人群包括 2766 名患者,他们分为两组:I 组(1553 名非糖尿病患者)和 II 组(1213 名患有 2 型 DM 的患者)。II 组患者随后分为两个亚组:IIA 亚组(981 名接受口服降糖药物治疗的患者)和 IIB 亚组(232 名接受胰岛素治疗的患者,无论是否同时使用额外的口服降糖药物)。评估了住院、1、3、5 和 10 年的死亡率结果变量。平均随访时间为 97±41 个月。
I 组和 II 组患者(1.87% vs. 2.31%,p=0.422)以及 IIA 和 IIB 亚组(2.14% vs. 3.02%,p=0.464)之间的住院死亡率相似。长期死亡率(1、3、5 和 10 年)在 II 组(2 型糖尿病)中高于 I 组(非糖尿病患者)(5.3% vs. 3.6%,p=0.038;9.3% vs. 5.6%,p<0.001;15.3% vs. 9.3%,p<0.001 和 47.3% vs. 29.6%,p<0.001)。Kaplan-Meier 分析表明,全因死亡率在 II 组中高于 I 组(p<0.001),在 IIB 亚组中高于 IIA 亚组(p=0.001)。多变量分析表明,DM 使死亡率的危险增加了一倍,而在糖尿病患者中,胰岛素治疗使死亡率的危险增加了一倍。
糖尿病和非糖尿病患者的住院死亡率相似。糖尿病患者的生存率在手术后 3 年开始恶化。2 型 DM 是单纯 CABG 手术后长期死亡率的独立预测因素。当糖尿病治疗策略包括胰岛素时,死亡率甚至更高。