Thoracic Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York; Department of Pathology, Beijing Chest Hospital, Capital Medical University, Beijing, China.
Thoracic Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York; Department of Pathology, Keio University School of Medicine, Tokyo, Japan.
J Thorac Oncol. 2019 Mar;14(3):482-493. doi: 10.1016/j.jtho.2018.11.017. Epub 2018 Nov 29.
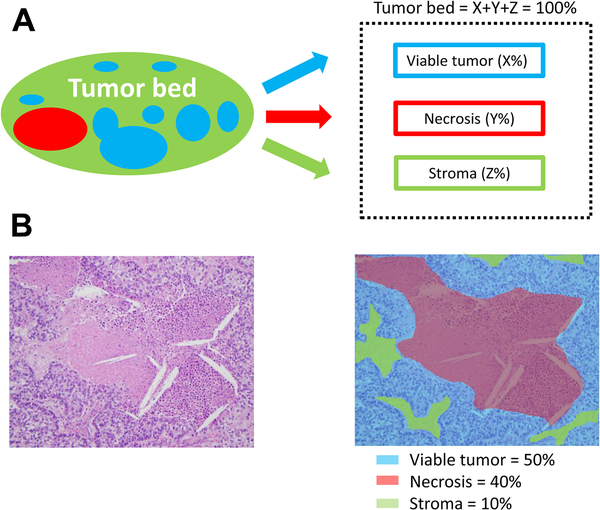
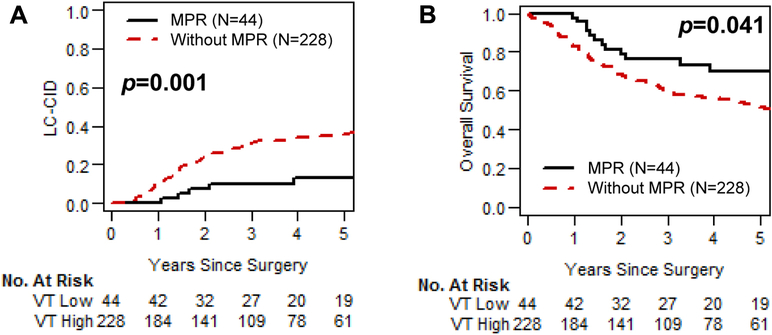
Major pathologic response after neoadjuvant chemotherapy (NAC) for NSCLC has been defined as 10% or less residual viable tumor without distinguishing between histologic types. We sought to investigate whether the optimal cutoff percentage of residual viable tumor for predicting survival differs between lung adenocarcinoma (ADC) and squamous cell carcinoma (SCC).
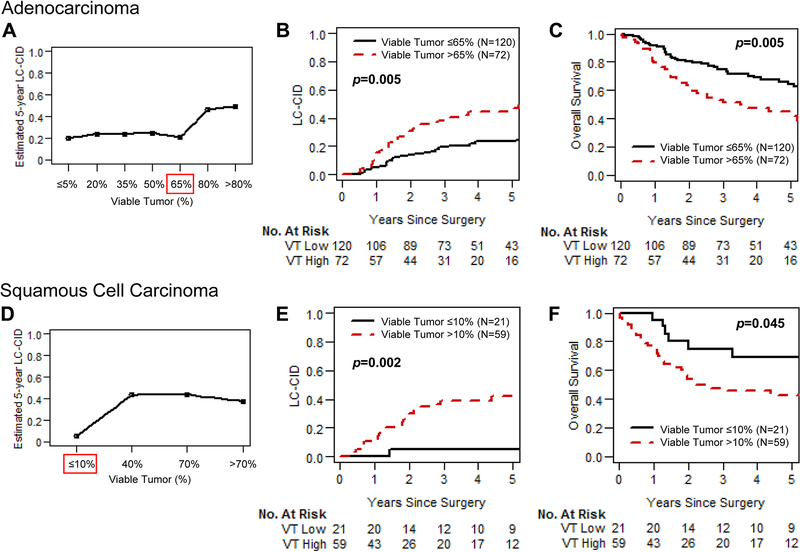
Tumor slides from 272 patients treated with NAC and surgery for clinical stage II-III NSCLC (ADC, n = 192; SCC, n = 80) were reviewed. The optimal cutoff percentage of viable tumor for predicting lung cancer-specific cumulative incidence of death (LC-CID) was determined using maximally selected rank statistics. LC-CID was analyzed using a competing-risks approach. Overall survival was evaluated using Kaplan-Meier methods and Cox proportional hazard analysis.
Patients with SCC had a better response to NAC (median percentage of viable tumor: SCC versus ADC, 40% versus 60%; p = 0.027). Major pathologic response (≤10% viable tumor) was observed in 26% of SCC cases versus 12% of ADC cases (p = 0.004). The optimal cutoff percentage of viable tumor for LC-CID was 10% for SCC and 65% for ADC. On multivariable analysis, viable tumor 10% or less was an independent factor for better LC-CID (p = 0.035) in patients with SCC; in patients with ADC, viable tumor 65% or less was a factor for better LC-CID (p = 0.033) and overall survival (p = 0.050).
In response to NAC, the optimal cutoff percentage of viable tumor for predicting survival differs between ADC and SCC. Our findings have implications for the pathologic assessment of resected specimens, especially in upcoming clinical trials design.
新辅助化疗(NAC)后非小细胞肺癌(NSCLC)的主要病理反应定义为 10%或更少的残留存活肿瘤,而没有区分组织学类型。我们试图研究预测生存的残留存活肿瘤的最佳截断百分比是否在肺腺癌(ADC)和鳞状细胞癌(SCC)之间存在差异。
对 272 例接受 NAC 和手术治疗的 II-III 期 NSCLC 患者(ADC,n=192;SCC,n=80)的肿瘤切片进行了回顾性研究。使用最大选择秩统计确定预测肺癌特异性累积死亡率(LC-CID)的最佳存活肿瘤百分比截断值。使用竞争风险方法分析 LC-CID。使用 Kaplan-Meier 方法和 Cox 比例风险分析评估总生存期。
SCC 患者对 NAC 的反应更好(存活肿瘤中位数百分比:SCC 与 ADC,40%与 60%;p=0.027)。SCC 病例中观察到主要病理反应(≤10%存活肿瘤)的比例为 26%,而 ADC 病例为 12%(p=0.004)。对于 SCC,LC-CID 的最佳存活肿瘤百分比截断值为 10%,对于 ADC,为 65%。多变量分析显示,SCC 患者中存活肿瘤 10%或更少是 LC-CID 更好的独立因素(p=0.035);在 ADC 患者中,存活肿瘤 65%或更少是 LC-CID 更好的因素(p=0.033)和总生存期(p=0.050)。
在 NAC 反应中,预测生存的残留存活肿瘤的最佳截断百分比在 ADC 和 SCC 之间存在差异。我们的研究结果对切除标本的病理评估具有重要意义,特别是在即将进行的临床试验设计中。