Department of Hematology, Seoul St. Mary's Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea.
Hematology Transplant Unit, Hôpital Saint-Louis, Paris, France.
Blood. 2019 Feb 7;133(6):530-539. doi: 10.1182/blood-2018-09-876136. Epub 2018 Dec 3.
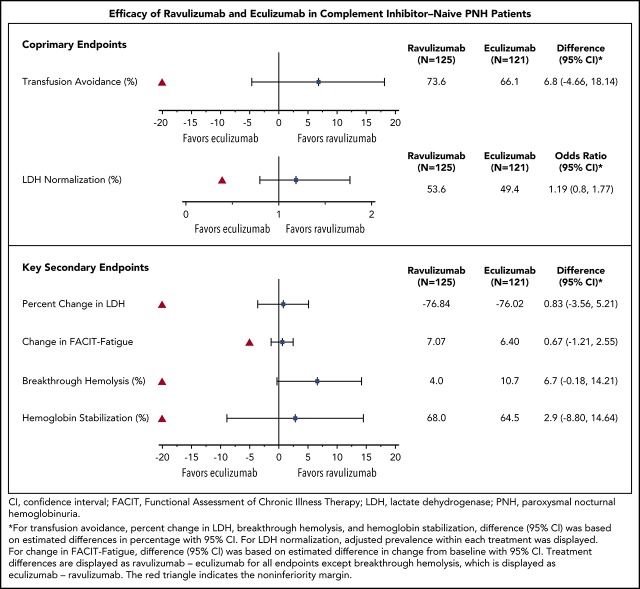
Ravulizumab (ALXN1210), a new complement C5 inhibitor, provides immediate, complete, and sustained C5 inhibition. This phase 3, open-label study assessed the noninferiority of ravulizumab to eculizumab in complement inhibitor-naive adults with paroxysmal nocturnal hemoglobinuria (PNH). Patients with lactate dehydrogenase (LDH) ≥1.5 times the upper limit of normal and at least 1 PNH symptom were randomized 1:1 to receive ravulizumab or eculizumab for 183 days (N = 246). Coprimary efficacy end points were proportion of patients remaining transfusion-free and LDH normalization. Secondary end points were percent change from baseline in LDH, change from baseline in Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue score, proportion of patients with breakthrough hemolysis, stabilized hemoglobin, and change in serum free C5. Ravulizumab was noninferior to eculizumab for both coprimary and all key secondary end points ( < .0001): transfusion avoidance (73.6% vs 66.1%; difference of 6.8% [95% confidence interval (CI), -4.66, 18.14]), LDH normalization (53.6% vs 49.4%; odds ratio, 1.19 [0.80, 1.77]), percent reduction in LDH (-76.8% vs -76.0%; difference [95% CI], -0.83% [-5.21, 3.56]), change in FACIT-Fatigue score (7.07 vs 6.40; difference [95% CI], 0.67 [-1.21, 2.55]), breakthrough hemolysis (4.0% vs 10.7%; difference [95% CI], -6.7% [-14.21, 0.18]), and stabilized hemoglobin (68.0% vs 64.5%; difference [95% CI], 2.9 [-8.80, 14.64]). The safety and tolerability of ravulizumab and eculizumab were similar; no meningococcal infections occurred. In conclusion, ravulizumab given every 8 weeks achieved noninferiority compared with eculizumab given every 2 weeks for all efficacy end points, with a similar safety profile. This trial was registered at www.clinicaltrials.gov as #NCT02946463.
拉维珠单抗(ALXN1210)是一种新型的补体 C5 抑制剂,可实现 C5 的即刻、完全和持续抑制。这项开放标签的 3 期研究评估了拉维珠单抗在补体抑制剂初治的阵发性睡眠性血红蛋白尿症(PNH)成人患者中的非劣效性,患者乳酸脱氢酶(LDH)≥正常上限的 1.5 倍且至少有 1 种 PNH 症状。患者按照 1:1 随机分组,分别接受拉维珠单抗或依库珠单抗治疗 183 天(N=246)。主要疗效终点为无输血和 LDH 正常化的患者比例。次要终点为 LDH 从基线的变化、慢性病治疗功能评估(FACIT)-疲劳评分的变化、突破性溶血、稳定血红蛋白和血清游离 C5 的变化。拉维珠单抗在所有主要和次要关键终点均非劣效于依库珠单抗(<0.0001):避免输血(73.6% vs 66.1%;差值为 6.8%[95%置信区间(CI),-4.66,18.14])、LDH 正常化(53.6% vs 49.4%;比值比,1.19[0.80,1.77])、LDH 从基线的减少百分比(-76.8% vs -76.0%;差值[95%CI],-0.83%[-5.21,3.56])、FACIT-Fatigue 评分的变化(7.07 vs 6.40;差值[95%CI],0.67[-1.21,2.55])、突破性溶血(4.0% vs 10.7%;差值[95%CI],-6.7%[-14.21,0.18])和稳定血红蛋白(68.0% vs 64.5%;差值[95%CI],2.9[-8.80,14.64])。拉维珠单抗和依库珠单抗的安全性和耐受性相似;未发生脑膜炎球菌感染。综上,与每 2 周给予依库珠单抗相比,每 8 周给予拉维珠单抗在所有疗效终点均达到非劣效性,且安全性特征相似。这项试验在 www.clinicaltrials.gov 上注册,编号为#NCT02946463。