Department of Haematological Medicine, King's College Hospital, National Institute of Health Research/Wellcome King's Clinical Research Facility, London, United Kingdom.
Department of Haematology, Leeds Teaching Hospitals, Leeds, United Kingdom.
Blood. 2019 Feb 7;133(6):540-549. doi: 10.1182/blood-2018-09-876805. Epub 2018 Dec 3.
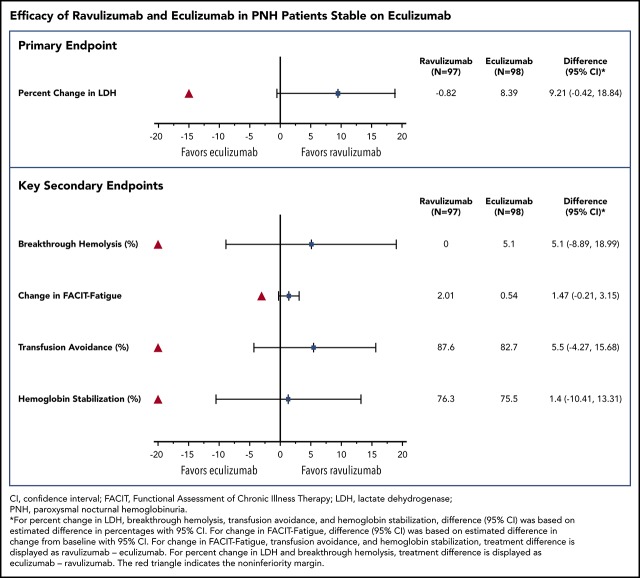
Ravulizumab, a new complement component C5 inhibitor administered every 8 weeks, was noninferior to eculizumab administered every 2 weeks in complement-inhibitor-naive patients with paroxysmal nocturnal hemoglobinuria (PNH). This study assessed noninferiority of ravulizumab to eculizumab in clinically stable PNH patients during previous eculizumab therapy. In this phase 3, open-label, multicenter study, 195 PNH patients on labeled-dose (900 mg every 2 weeks) eculizumab for >6 months were randomly assigned 1:1 to switch to ravulizumab (n = 97) or continue eculizumab (n = 98). Primary efficacy end point was percentage change in lactate dehydrogenase (LDH) from baseline to day 183. Key secondary end points included proportion of patients with breakthrough hemolysis, change in Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue score, transfusion avoidance, and stabilized hemoglobin. In 191 patients completing 183 days of treatment, ravulizumab was noninferior to eculizumab ( < .0006 for all end points), including percentage change in LDH (difference, 9.21% [95% confidence interval (CI), -0.42 to 18.84], = .058 for superiority), breakthrough hemolysis (difference, 5.1 [95% CI, -8.89 to 18.99]), change in FACIT-Fatigue score (difference, 1.47 [95% CI, -0.21 to 3.15]), transfusion avoidance (difference, 5.5 [95% CI, -4.27 to 15.68]), and stabilized hemoglobin (difference, 1.4 [95% CI, -10.41 to 13.31]). The most frequently reported adverse event was headache (26.8%, ravulizumab; 17.3%, eculizumab). No meningococcal infections or discontinuations due to adverse events occurred. Patients with PNH may be safely and effectively switched from labeled-dose eculizumab administered every 2 weeks to ravulizumab administered every 8 weeks. This trial was funded by Alexion Pharmaceuticals, Inc., and is registered at www.clinicaltrials.gov as #NCT03056040.
拉维珠单抗是一种新型补体成分 C5 抑制剂,每 8 周给药 1 次,在补体抑制剂初治的阵发性夜间血红蛋白尿(PNH)患者中与每 2 周给药 1 次的依库珠单抗相比非劣效。这项研究评估了拉维珠单抗在接受依库珠单抗治疗的稳定 PNH 患者中的非劣效性。在这项 3 期、开放标签、多中心研究中,195 名接受标签剂量(每 2 周 900mg)依库珠单抗治疗超过 6 个月的 PNH 患者按 1:1 随机分配至拉维珠单抗组(n=97)或继续接受依库珠单抗组(n=98)。主要疗效终点为从基线到第 183 天乳酸脱氢酶(LDH)的百分比变化。关键次要终点包括突破性溶血的患者比例、慢性疾病治疗功能评估(FACIT)-疲劳评分的变化、输血回避和稳定的血红蛋白。在完成 183 天治疗的 191 名患者中,拉维珠单抗非劣效于依库珠单抗(所有终点均<.0006),包括 LDH 的百分比变化(差异,9.21%[95%CI,-0.42 至 18.84],=.058 为优效性)、突破性溶血(差异,5.1[95%CI,-8.89 至 18.99])、FACIT-Fatigue 评分的变化(差异,1.47[95%CI,-0.21 至 3.15])、输血回避(差异,5.5[95%CI,-4.27 至 15.68])和稳定的血红蛋白(差异,1.4[95%CI,-10.41 至 13.31])。最常报告的不良事件是头痛(26.8%,拉维珠单抗;17.3%,依库珠单抗)。没有发生脑膜炎球菌感染或因不良事件停药。接受 PNH 治疗的患者可以安全有效地从每 2 周给药的标签剂量依库珠单抗转换为每 8 周给药的拉维珠单抗。这项试验由 Alexion 制药公司资助,并在 www.clinicaltrials.gov 上注册,编号为 #NCT03056040。