Department of Radiology, Seoul National University Hospital, Seoul, Korea.
Department of Radiology, Seoul National University College of Medicine, Seoul, Korea.
PLoS One. 2018 Dec 5;13(12):e0207880. doi: 10.1371/journal.pone.0207880. eCollection 2018.
To investigate the imaging features of cyst infection in autosomal dominant polycystic kidney disease (ADPKD) patients using computed tomography (CT) and ultrasonography (US).
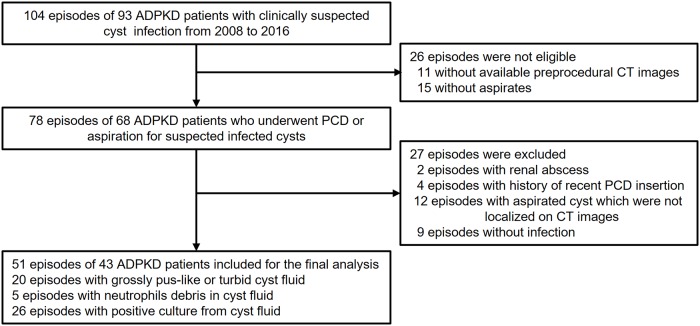
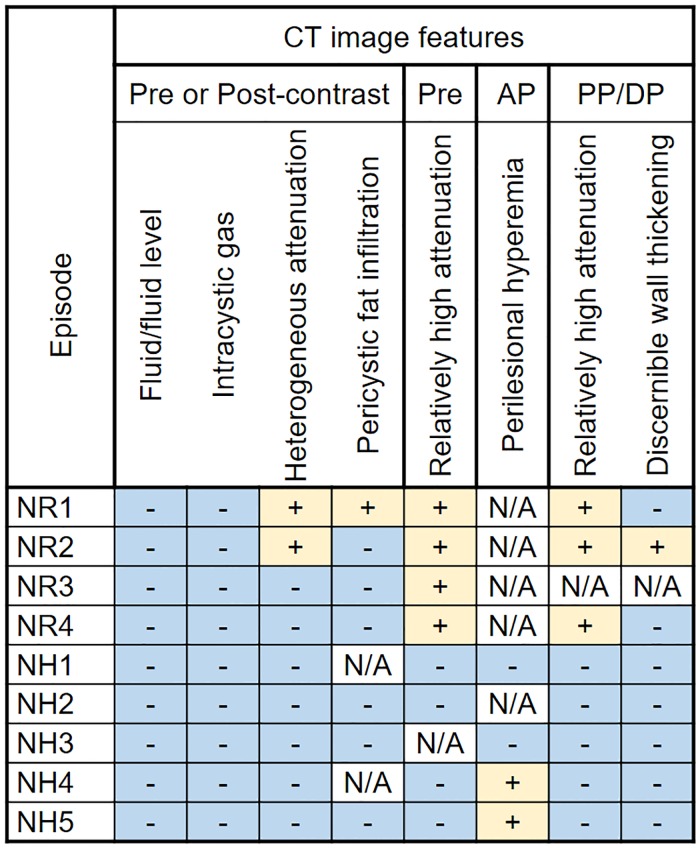
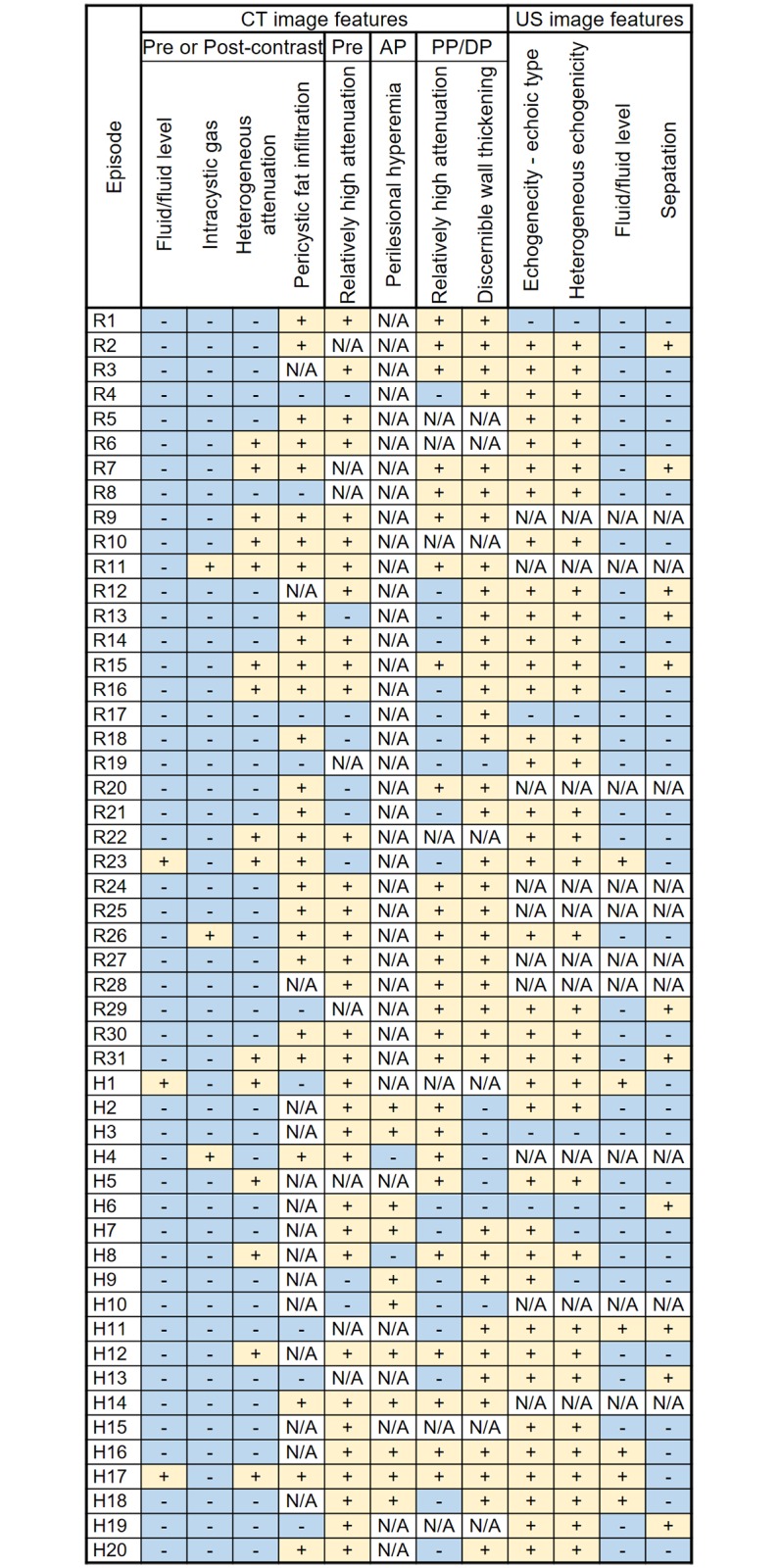
MATERIALS & METHODS: The institutional review board approved this retrospective study. Fifty-one episodes with proven cyst infection in forty-three ADPKD patients were included. Two experienced abdominal radiologists reviewed CT and US images and evaluated the following imaging features in consensus: cyst size, location, cyst shape, intracystic attenuation, intracystic echogenicity, intracystic heterogeneity, wall thickness, the presence of fluid-fluid level, septation, intracystic gas, pericystic fat infiltration, and pericystic hyperemia. Intracystic attenuation was measured for all infected cysts and two presumed normal cysts and compared using the Wilcoxon rank-sum test.
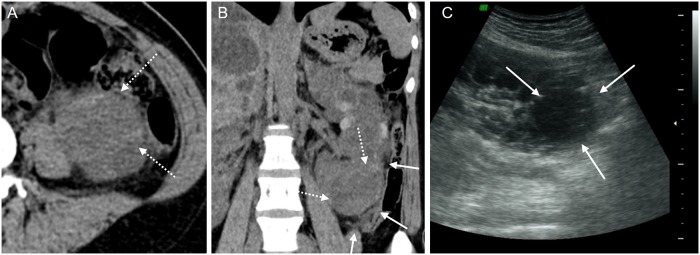
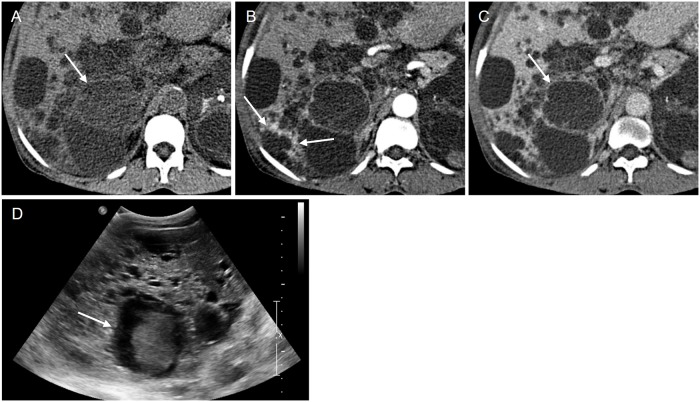
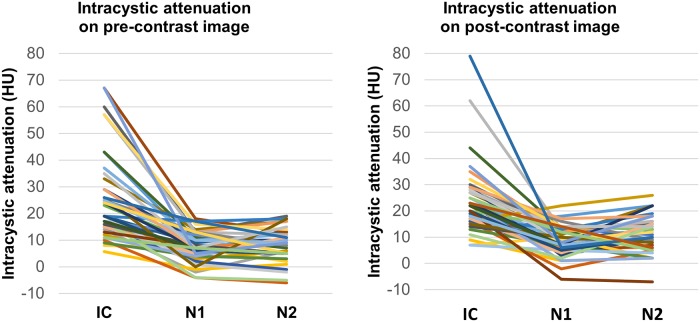
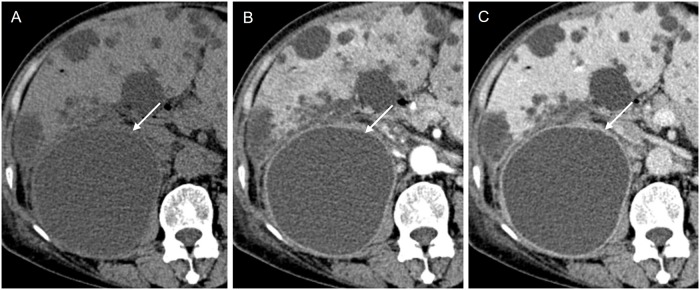
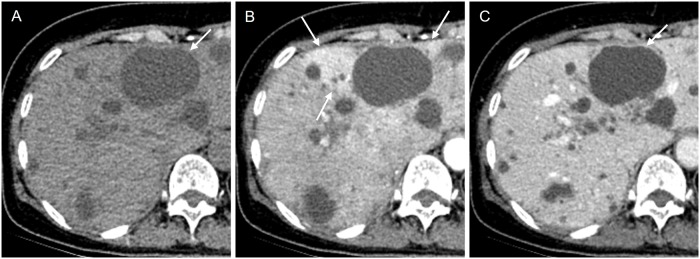
On CT scans, the median size of infected cysts was 5.5 cm (range: 2.3-18.8 cm) and 46 of 51 (90.2%) infected cysts were located in the subcapsular region. Most (48 of 51, 94.1%) infected cysts showed lobulated, focal bulging or irregular shape. Discernible wall thickening (84.1%) was the most frequently found imaging feature of infected cysts followed by relatively higher intracystic attenuation compared to normal cysts (79.1%) and pericystic fat infiltration (52.9%). Fluid/fluid level was found in 3 of 51 (5.9%) infected cysts and intracystic gas was found in 3 of 51 (5.9%) infected cysts, respectively. For hepatic cysts, 11 of 14 (78.6%) infected cysts showed pericystic hyperemia. Intracystic attenuation was significantly higher in infected cysts (median; 19.0 HU) than in presumed normal cysts (median; 8.5 HU) (P<0.001), and exceeded 25 HU in 18 (35.3%) of 51 infected cysts. Among the 41 infected cysts for which US images were available, 35 (85.1%) showed heterogeneous echogenicity.
Minute imaging features such as minimal wall thickening or relatively high attenuation compared to normal cysts would be helpful to detect infected cysts in ADPKD patients.
利用计算机断层扫描(CT)和超声检查(US)研究常染色体显性多囊肾病(ADPKD)患者的囊肿感染的影像学特征。
本回顾性研究经机构审查委员会批准。共纳入 43 例 ADPKD 患者 51 例经证实的囊肿感染。两位经验丰富的腹部放射科医生对 CT 和 US 图像进行了审查,并通过共识评估了以下影像学特征:囊肿大小、位置、囊肿形状、囊内衰减、囊内回声、囊内异质性、囊壁厚度、存在液-液平面、分隔、囊内气体、囊周脂肪浸润和囊周充血。对所有感染性囊肿和两个假定的正常囊肿均测量了囊内衰减,并使用 Wilcoxon 秩和检验进行比较。
在 CT 扫描上,感染性囊肿的中位数大小为 5.5cm(范围:2.3-18.8cm),51 个感染性囊肿中有 46 个(90.2%)位于包膜下区域。大多数(48/51,94.1%)感染性囊肿呈分叶状、局灶性膨出或不规则形状。最常发现的感染性囊肿影像学特征是囊壁增厚(84.1%),其次是与正常囊肿相比相对较高的囊内衰减(79.1%)和囊周脂肪浸润(52.9%)。3 个(5.9%)感染性囊肿中有 3 个存在液-液平面,3 个(5.9%)感染性囊肿中有 3 个存在囊内气体。在 14 个肝囊肿中,11 个(78.6%)感染性囊肿有囊周充血。感染性囊肿的囊内衰减明显高于假定的正常囊肿(中位数;19.0HU)(P<0.001),51 个感染性囊肿中有 18 个(35.3%)的囊内衰减超过 25HU。在有 US 图像的 41 个感染性囊肿中,35 个(85.1%)显示出不均匀的回声。
与正常囊肿相比,微小的影像学特征,如最小的囊壁增厚或相对较高的衰减,有助于检测 ADPKD 患者的感染性囊肿。