Center for Pulmonary Vascular Diseases, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, 167 Beilishi Road, Xicheng District, Beijing, 100037, China.
BMC Cardiovasc Disord. 2018 Dec 10;18(1):229. doi: 10.1186/s12872-018-0953-7.
Takotsubo syndrome (TTS) is an acute cardiac condition with reversible heart failure which is often triggered by psychological and physical stressful events. Although pulmonary embolism (PE) was reported as a trigger for TTS, the concurrence of TTS and PE has been rarely reported, let alone that triggered by PE. Here we describe a case of a postmenopausal female presenting with symptoms similar to myocardial ischemia, which may be caused by PE, and review the available literature that may help clinicians with their practice to similar situations since no published guidelines are available.
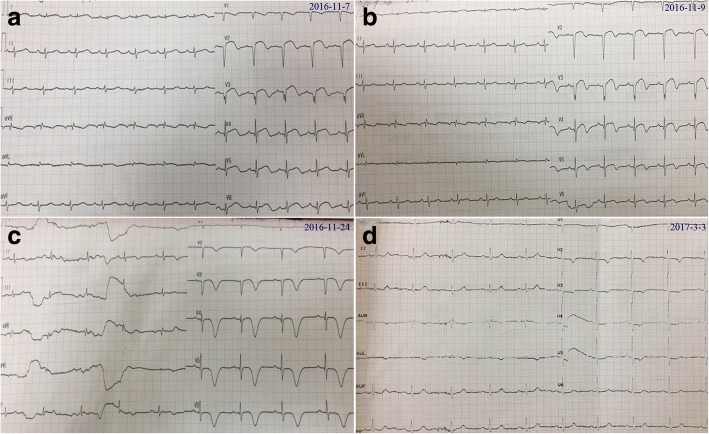
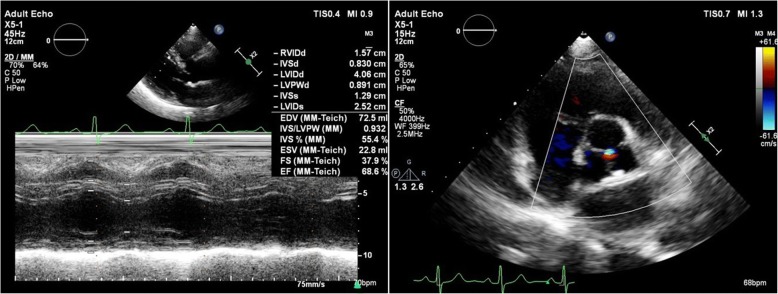
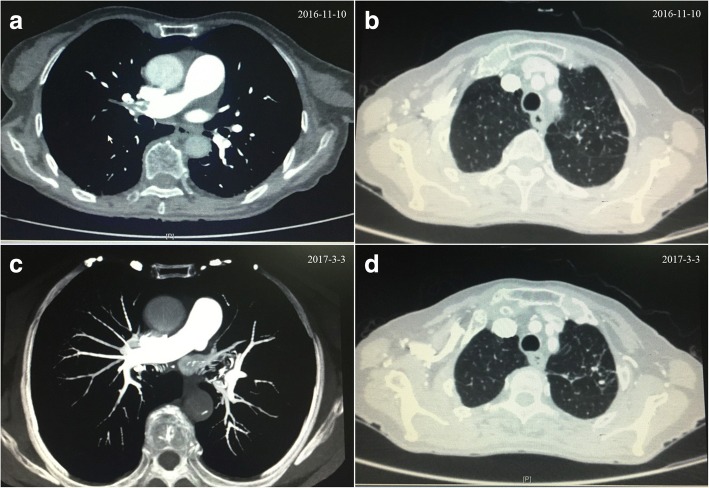
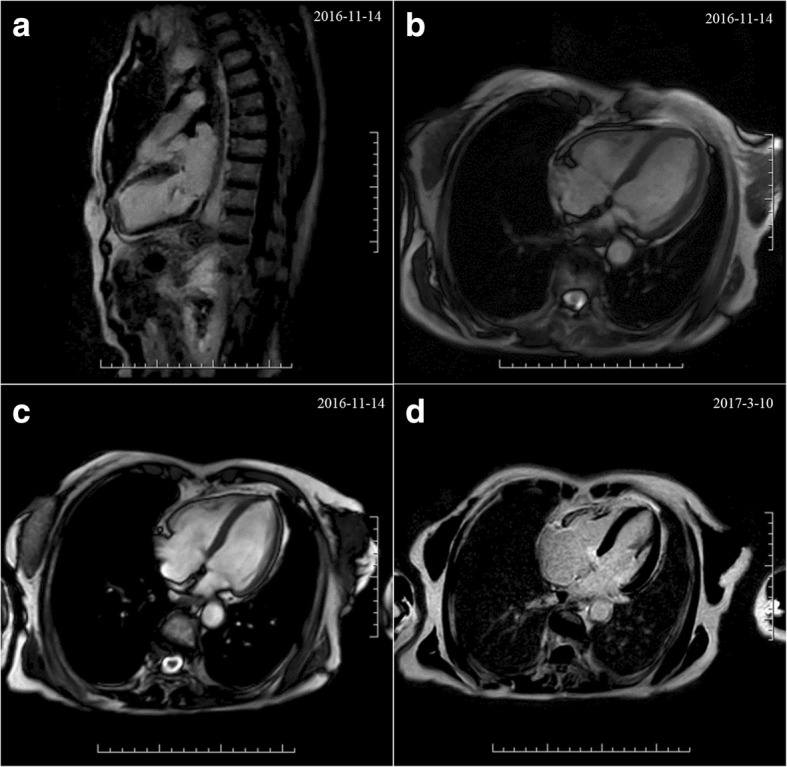
An 86-year-old female was referred to the emergency department for unrelieved chest tightness, shortness of breath and back pain. Cardiac biomarkers were mildly elevated and electrocardiogram displayed pathologic Q-waves, ST-segment elevation and inverted T-waves. Unexpectedly, coronary angiography was in absence of obstructed coronary atherosclerosis or acute plaque rupture. Chest computed tomography illustrated multiple pulmonary emboli in bilateral pulmonary arteries. She had suffered from long-term right lower extremity pain and experienced a long railway journey with less activity. Both echocardiogram and cardiac magnetic resonance demonstrated regional hypokinesia of left ventricle. She received anticoagulant and diuretic therapies, three-month follow up after discharge revealed uneventful recovery without any pulmonary emboli or regional motion abnormalities, thus she was retrospectively diagnosed with TTS caused by PE.
TTS and PE are scarcely concurrent and PE can exert as a potential trigger for TTS. TTS is easily misdiagnosed, actively seeking possible risk factors of TTS is in favor of early diagnosis and timely intervention. TTS with PE is reversible, timely and effective treatments ensure the best possible outcome.
Takotsubo 综合征(TTS)是一种伴有可逆性心力衰竭的急性心脏疾病,常由心理和身体应激事件引发。尽管已有报道称肺栓塞(PE)可引发 TTS,但 TTS 与 PE 同时发生的情况很少见,更不用说由 PE 引发的 TTS 了。在这里,我们描述了一例绝经后女性出现类似心肌缺血的症状,可能由 PE 引起,并回顾了现有的文献,这可能有助于临床医生在遇到类似情况时进行实践,因为目前尚无相关指南。
一名 86 岁女性因持续性胸痛、呼吸困难和背痛被转诊至急诊科。心脏生物标志物轻度升高,心电图显示病理性 Q 波、ST 段抬高和 T 波倒置。出乎意料的是,冠状动脉造影未见阻塞性冠状动脉粥样硬化或急性斑块破裂。胸部计算机断层扫描显示双侧肺动脉多发性肺栓塞。她长期右下肢疼痛,且经历了一次长途铁路旅行,活动量较少。超声心动图和心脏磁共振均显示左心室区域性运动减弱。她接受了抗凝和利尿剂治疗,出院后 3 个月随访显示无不良事件,无肺栓塞或区域性运动异常,因此回顾性诊断为由 PE 引起的 TTS。
TTS 和 PE 很少同时发生,PE 可能作为 TTS 的潜在触发因素。TTS 易误诊,积极寻找 TTS 的可能危险因素有助于早期诊断和及时干预。PE 合并 TTS 是可逆的,及时有效的治疗可确保最佳预后。