Moman Rajat N, Ostby Stuart A, Akhoundi Abbasali, Kashyap Rahul, Kashani Kianoush
Multidisciplinary Epidemiology and Translational Research in Intensive Care (METRIC), Division of Pulmonary and Critical Care Medicine, Department of Medicine, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, MN, USA.
Ann Intensive Care. 2018 Dec 10;8(1):124. doi: 10.1186/s13613-018-0468-5.
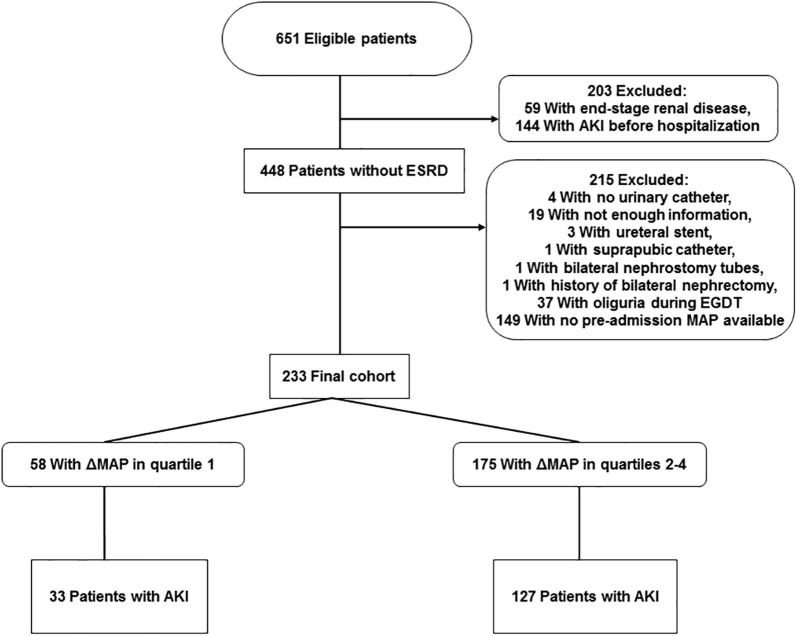
To examine the relationship between delta mean arterial pressure (ΔMAP; MAP change between pre-admission minus post-resuscitation) and acute kidney injury (AKI) among patients with septic shock. In this retrospective, single-center cohort study of adult patients pre-admission MAP is defined as the median MAP recorded from 365 to 7 days before admission. Post-resuscitation MAP was median MAP during the 7th hour after initiating resuscitation.
In our cohort (N = 233; 55% male), the median (interquartile range [IQR]) age was 71 (58-81) years and the median (IQR) acute physiology, age, chronic health evaluation (APACHE) III score was 81 (66-97). Although those in the lowest ΔMAP quartile (-24.5 to 3.9 mmHg) had no demographic differences compared with the rest of the cohort, the odds ratio for AKI was 0.26 (95% CI 0.11-0.57) after adjustment for other known AKI risk factors. Among patients with a history of hypertension, the lowest quartile had an odds ratio for AKI of 0.12 (95% CI 0.04-0.37) after adjusting for risk factors for AKI in this cohort.
The incidence of AKI was lowest among those whose post-resuscitation MAP was closest to or higher than their pre-admission MAP. Further study regarding the effect of targeting the pre-admission MAP for post-resuscitation on the incidence of AKI is warranted.
探讨脓毒性休克患者的平均动脉压变化值(ΔMAP;入院前与复苏后MAP的差值)与急性肾损伤(AKI)之间的关系。在这项针对成年患者的回顾性单中心队列研究中,入院前MAP定义为入院前365天至7天记录的MAP中位数。复苏后MAP为开始复苏后第7小时的MAP中位数。
在我们的队列(N = 233;55%为男性)中,年龄中位数(四分位间距[IQR])为71(58 - 81)岁,急性生理功能、年龄、慢性健康状况评估(APACHE)III评分中位数(IQR)为81(66 - 97)。尽管最低ΔMAP四分位数组(-24.5至3.9 mmHg)与队列其他患者相比在人口统计学上无差异,但在调整其他已知的AKI危险因素后,AKI的比值比为0.26(95%CI 0.11 - 0.57)。在有高血压病史的患者中,在调整该队列中AKI的危险因素后,最低四分位数组AKI的比值比为0.12(95%CI 0.04 - 0.37)。
复苏后MAP最接近或高于入院前MAP的患者中,AKI的发生率最低。有必要进一步研究将复苏后MAP目标设定为入院前MAP对AKI发生率的影响。