Poukkanen Meri, Wilkman Erika, Vaara Suvi T, Pettilä Ville, Kaukonen Kirsi-Maija, Korhonen Anna-Maija, Uusaro Ari, Hovilehto Seppo, Inkinen Outi, Laru-Sompa Raili, Hautamäki Raku, Kuitunen Anne, Karlsson Sari
Crit Care. 2013 Dec 13;17(6):R295. doi: 10.1186/cc13161.
Knowledge of the association of hemodynamics with progression of septic acute kidney injury (AKI) is limited. However, some recent data suggest that mean arterial pressure (MAP) exceeding current guidelines (60-65 mmHg) may be needed to prevent AKI. We hypothesized that higher MAP during the first 24 hours in the intensive care unit (ICU), would be associated with a lower risk of progression of AKI in patients with severe sepsis.
We identified 423 patients with severe sepsis and electronically recorded continuous hemodynamic data in the prospective observational FINNAKI study. The primary endpoint was progression of AKI within the first 5 days of ICU admission defined as new onset or worsening of AKI by the Kidney Disease: Improving Global Outcomes (KDIGO) criteria. We evaluated the association of hemodynamic variables with this endpoint. We included 53724 10-minute medians of MAP in the analysis. We analysed the ability of time-adjusted MAP to predict progression of AKI by receiver operating characteristic (ROC) analysis.
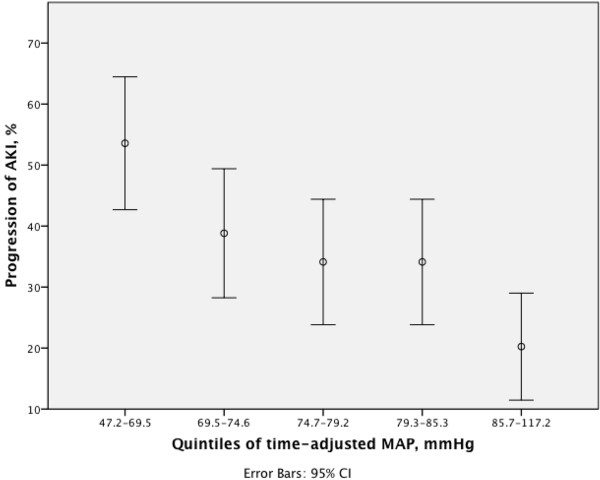
Of 423 patients, 153 (36.2%) had progression of AKI. Patients with progression of AKI had significantly lower time-adjusted MAP, 74.4 mmHg [68.3-80.8], than those without progression, 78.6 mmHg [72.9-85.4], P < 0.001. A cut-off value of 73 mmHg for time-adjusted MAP best predicted the progression of AKI. Chronic kidney disease, higher lactate, higher dose of furosemide, use of dobutamine and time-adjusted MAP below 73 mmHg were independent predictors of progression of AKI.
The findings of this large prospective multicenter observational study suggest that hypotensive episodes (MAP under 73 mmHg) are associated with progression of AKI in critically ill patients with severe sepsis.
关于血流动力学与脓毒症急性肾损伤(AKI)进展之间关联的认识有限。然而,最近的一些数据表明,可能需要使平均动脉压(MAP)超过当前指南(60 - 65 mmHg)以预防AKI。我们假设,在重症监护病房(ICU)的最初24小时内维持较高的MAP,将与严重脓毒症患者AKI进展风险较低相关。
在一项前瞻性观察性FINNAKI研究中,我们纳入了423例严重脓毒症患者,并以电子方式记录连续的血流动力学数据。主要终点是ICU入院后前5天内AKI的进展,根据肾脏病改善全球预后(KDIGO)标准定义为AKI的新发或恶化。我们评估了血流动力学变量与该终点之间的关联。分析中纳入了53724个10分钟的MAP中位数。我们通过受试者工作特征(ROC)分析评估时间校正MAP预测AKI进展的能力。
在423例患者中,153例(36.2%)出现AKI进展。AKI进展患者的时间校正MAP显著低于未进展患者,分别为74.4 mmHg [68.3 - 80.8]和78.6 mmHg [72.9 - 85.4],P < 0.001。时间校正MAP的截断值为73 mmHg时,对AKI进展的预测效果最佳。慢性肾脏病、较高的乳酸水平、较高剂量的呋塞米、使用多巴酚丁胺以及时间校正MAP低于73 mmHg是AKI进展的独立预测因素。
这项大型前瞻性多中心观察性研究的结果表明,低血压发作(MAP低于73 mmHg)与严重脓毒症重症患者的AKI进展相关。