Lin Chin-Yu, Lin Yenn-Jiang, Narayan Sanjiv M, Baykaner Tina, Lo Men-Tzung, Chung Fa-Po, Chen Yun-Yu, Chang Shih-Lin, Lo Li-Wei, Hu Yu-Feng, Liao Jo-Nan, Tuan Ta-Chuan, Chao Tze-Fan, Te Abigail Louise D, Kuo Ling, Vicera Jennifer Jeanne B, Chang Ting-Yung, Salim Simon, Chien Kuo-Liong, Chen Shih-Ann
Institute of Clinical Medicine, and Cardiovascular Research Center, National Yang-Ming University, Taipei City, Taiwan.
Division of Cardiology, Department of Medicine, Heart Rhythm Center, Taipei Veterans General Hospital, Taipei City, Taiwan.
Pacing Clin Electrophysiol. 2019 Feb;42(2):216-223. doi: 10.1111/pace.13573. Epub 2018 Dec 27.
Adjunctive driver-guided ablation in addition to pulmonary vein isolation has been proposed as a strategy to improve procedural success and outcomes for various populations with atrial fibrillation (AF). First, this study aimed to evaluate the different mapping techniques for driver/rotor identification and second to evaluate the benefits of driver/rotor-guided ablation in patients with paroxysmal and persistent AF (PerAF).
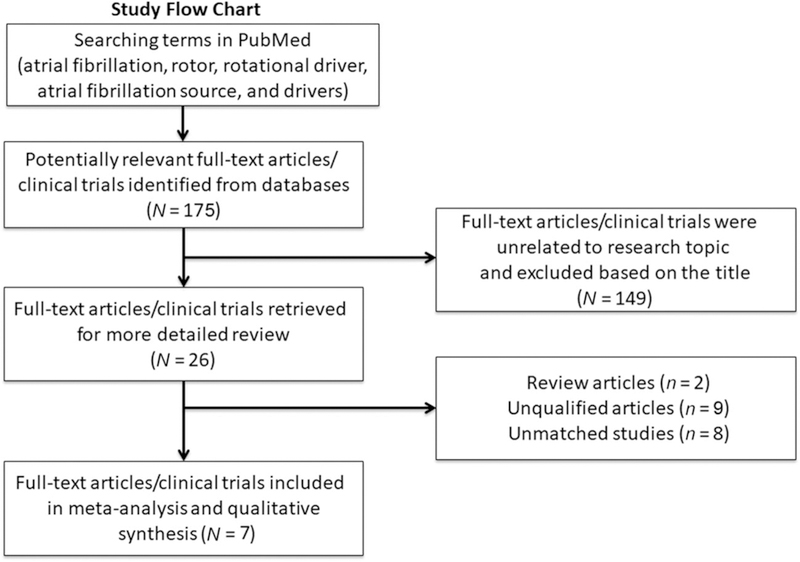
We searched the electronic database in PubMed using the keywords "atrial fibrillation," "rotor," "rotational driver," "atrial fibrillation source," and "drivers" for both randomized controlled trials and observational controlled trials. Clinical studies reporting efficacy or safety outcomes of driver-guided ablation for paroxysmal AF or (PerAF) were identified. We performed subgroup analyses comparing different driver mapping methods in patients with PerAF. The odds ratios (ORs) with random effects were analyzed.
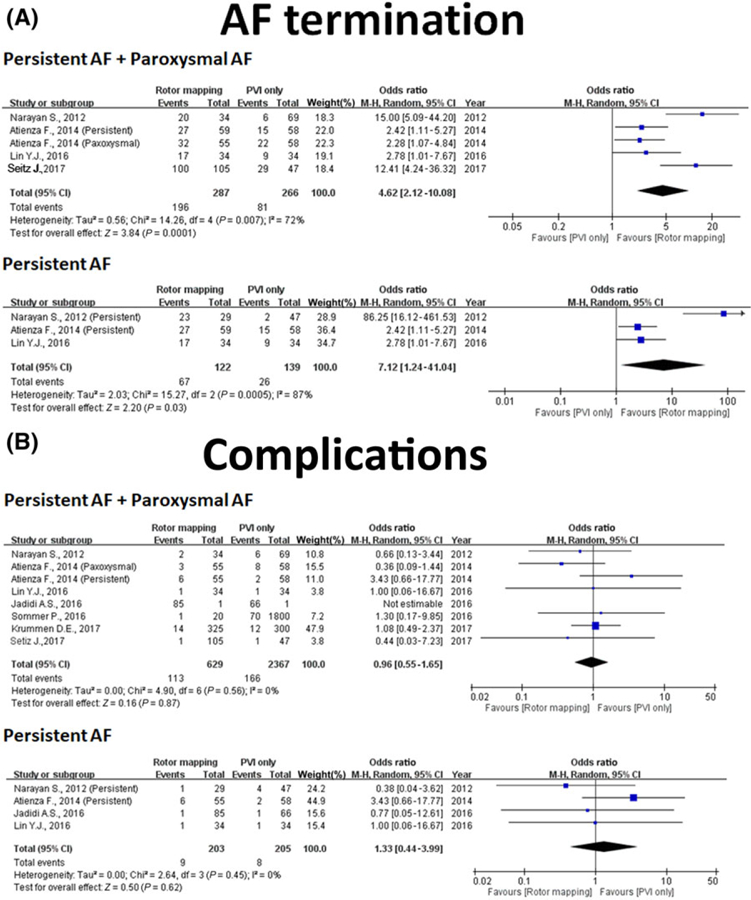
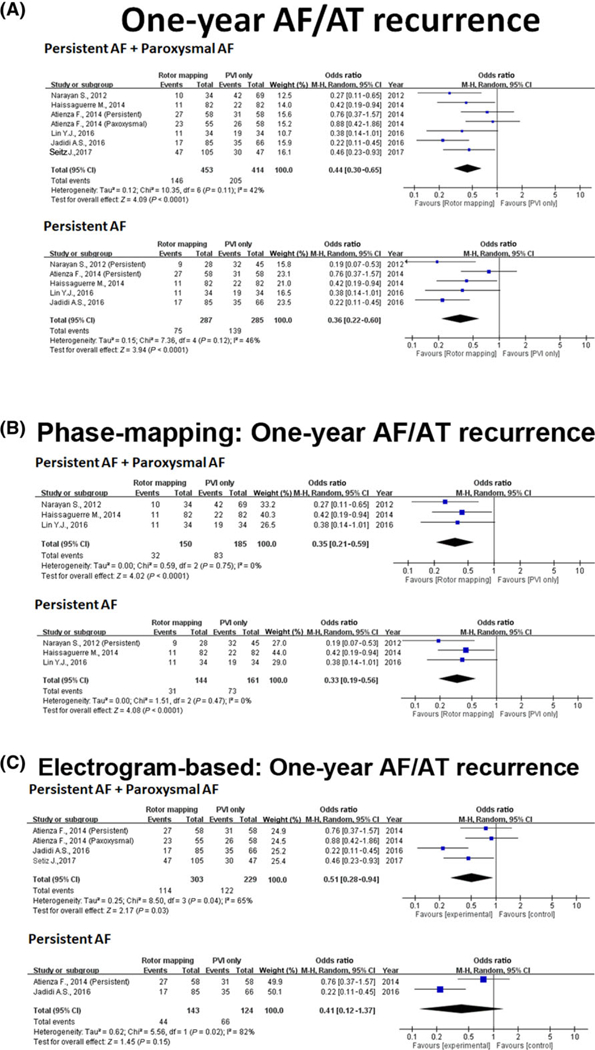
Out of 175 published articles, seven met the inclusion criteria, of which two were randomized controlled trials, one was quasiexperimental study, and four observational studies (three case-controlled studies and one cross-sectional study). Overall, adjunctive driver-guided ablation was associated with higher rates of acute AF termination (OR: 4.62, 95% confidence interval [CI]: 2.12-10.08; P < 0.001), lower recurrence of any atrial arrhythmia (OR: 0.44, 95% CI: 0.30-0.065; P < 0.001), and comparable complication incidence.
Adjunctive driver-guided catheter ablation suggested an increased freedom from AF/AT relative to conventional strategies, irrespective of the mapping techniques. Furthermore, phase mapping appears to be superior to electrogram-based driver mapping in PerAF ablation.
除肺静脉隔离外,辅助性驱动子引导下的消融术已被提出作为一种提高不同类型心房颤动(AF)患者手术成功率和治疗效果的策略。首先,本研究旨在评估用于识别驱动子/转子的不同标测技术,其次评估驱动子/转子引导下的消融术对阵发性和持续性房颤(PerAF)患者的益处。
我们在PubMed电子数据库中使用关键词“心房颤动”“转子”“旋转驱动子”“房颤起源”和“驱动子”搜索随机对照试验和观察性对照试验。确定报告驱动子引导下对阵发性房颤或(PerAF)消融术疗效或安全性结果的临床研究。我们进行亚组分析,比较PerAF患者中不同的驱动子标测方法。分析随机效应的优势比(OR)。
在175篇已发表的文章中,7篇符合纳入标准,其中2篇为随机对照试验,1篇为准实验研究,4篇为观察性研究(3篇病例对照研究和1篇横断面研究)。总体而言,辅助性驱动子引导下的消融术与更高的急性房颤终止率相关(OR:4.62,95%置信区间[CI]:2.12 - 10.08;P < 0.001),任何房性心律失常的复发率更低(OR:0.44,95% CI:0.30 - 0.065;P < 0.001),且并发症发生率相当。
辅助性驱动子引导下的导管消融术表明,相对于传统策略,房颤/房性心动过速(AT)发作的自由度增加,与标测技术无关。此外,在PerAF消融术中,相位标测似乎优于基于体表心电图的驱动子标测。