Chang Ting-Yung, Lin Chin-Yu, Lin Yenn-Jiang, Wu Cheng-I, Chang Shih-Lin, Lo Li-Wei, Hu Yu-Feng, Chung Fa-Po, Tuan Ta-Chuan, Chao Tze-Fan, Liao Jo-Nan, Kuo Ling, Liu Chih-Min, Chen Shih-Ann
Heart Rhythm Center, Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
Division of Cardiology, Taipei Veterans General Hospital, Taipei, Taiwan.
Heart Rhythm O2. 2022 Apr 19;3(3):269-278. doi: 10.1016/j.hroo.2022.04.003. eCollection 2022 Jun.
Catheter ablation is a current therapeutic approach for atrial fibrillation (AF). However, its efficacy for long-standing persistent AF remains suboptimal.
The purpose of this study was to test the hypothesis that a panoramic mapping system (CARTOFINDER, Biosense Webster) can guide pulmonary vein (PV) isolation and additional potential AF drivers.
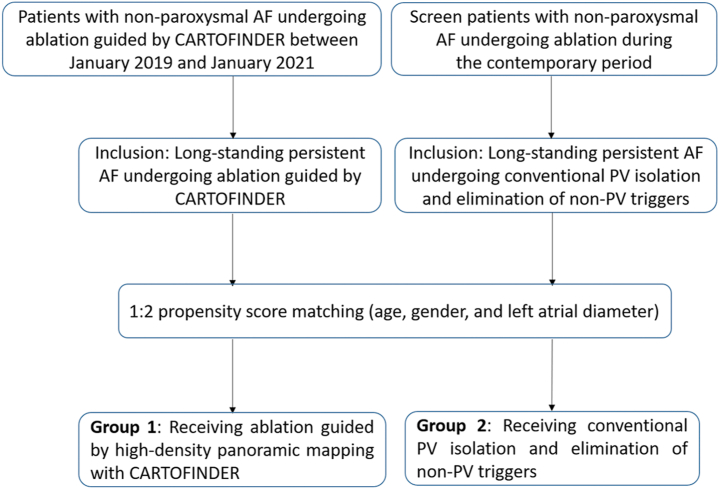
A total of 76 patients with nonparoxysmal AF referred for ablation guided by a novel high-density panoramic mapping system with CARTOFINDER were prospectively enrolled. Of this cohort, 40 patients (52.6%) had long-standing persistent AF (CARTOFINDER group). We then retrospectively screened the patients with long-standing persistent AF undergoing conventional PV isolation and elimination of non-PV triggers during the contemporary period (conventional group). They were matched at a 1:2 ratio (40 patients in group 1 received ablation guided by CARTOFINDER; 80 patients in group 2 receiving conventional PV isolation and elimination of non-PV triggers).
During follow-up, patients in group 1 had a lower recurrence AF rate than those in group 2 ( = .040). There was no difference in recurrence of atrial flutter ( = .996) and atrial tachycardia ( = .525). In Cox proportional hazards regression analysis, AF duration and PV isolation along with AF driver ablation using a panoramic mapping system with CARTOFINDER both were independent predictors of recurrent AF after catheter ablation of long-standing persistent AF.
Identification of the potential drivers in long-standing AF is crucial. Compared with conventional PV isolation and elimination of non-PV triggers, ablation guided by a high-density panoramic mapping system (CARTOFINDER) might have a better outcome in patients with long-standing persistent AF.
导管消融是目前治疗心房颤动(AF)的一种方法。然而,其对长期持续性房颤的疗效仍不理想。
本研究旨在验证以下假设,即全景标测系统(CARTOFINDER,Biosense Webster公司)可指导肺静脉(PV)隔离及其他潜在的房颤驱动因素。
前瞻性纳入76例接受由配备CARTOFINDER的新型高密度全景标测系统指导下进行消融的非阵发性房颤患者。在该队列中,40例患者(52.6%)患有长期持续性房颤(CARTOFINDER组)。然后,我们回顾性筛选了同期接受传统PV隔离及消除非PV触发因素的长期持续性房颤患者(传统组)。两组按1:2比例匹配(第1组40例患者接受CARTOFINDER指导下的消融;第2组80例患者接受传统PV隔离及消除非PV触发因素)。
随访期间,第1组患者的房颤复发率低于第2组(P = 0.040)。心房扑动(P = 0.996)和房性心动过速(P = 0.525)的复发情况无差异。在Cox比例风险回归分析中,房颤持续时间、PV隔离以及使用配备CARTOFINDER的全景标测系统进行房颤驱动因素消融均是长期持续性房颤导管消融术后房颤复发的独立预测因素。
识别长期房颤中的潜在驱动因素至关重要。与传统PV隔离及消除非PV触发因素相比,由高密度全景标测系统(CARTOFINDER)指导的消融对于长期持续性房颤患者可能具有更好的疗效。