Timmers Inge, Park Anna L, Fischer Molly D, Kronman Corey A, Heathcote Lauren C, Hernandez J Maya, Simons Laura E
Department of Anesthesiology, Perioperative, and Pain Medicine, Stanford University School of Medicine, Palo Alto, CA, United States.
Front Behav Neurosci. 2018 Nov 27;12:289. doi: 10.3389/fnbeh.2018.00289. eCollection 2018.
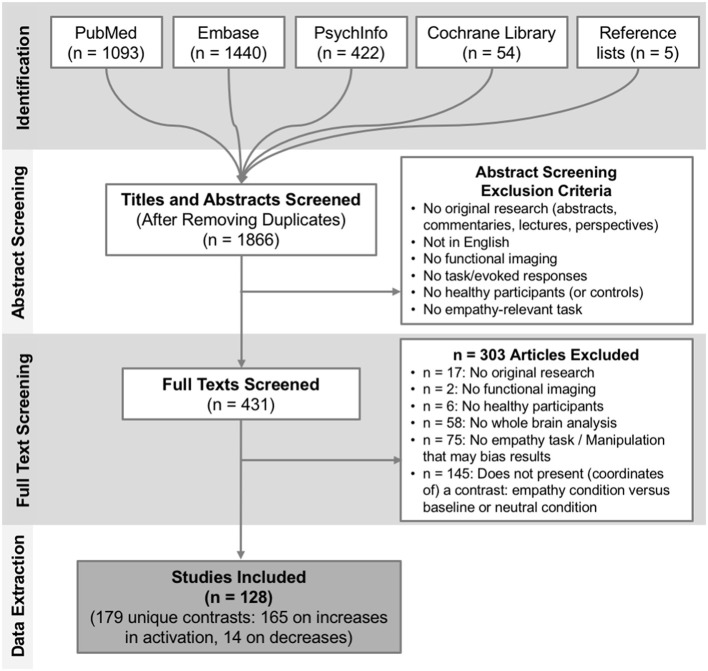
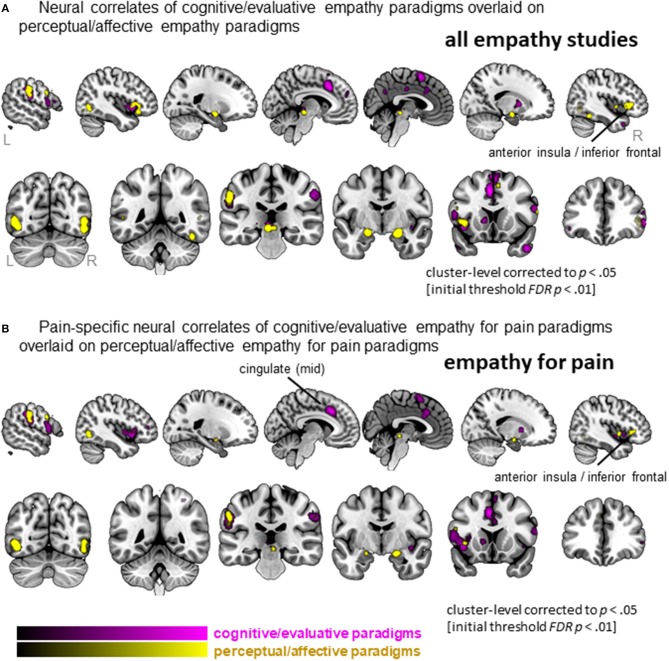
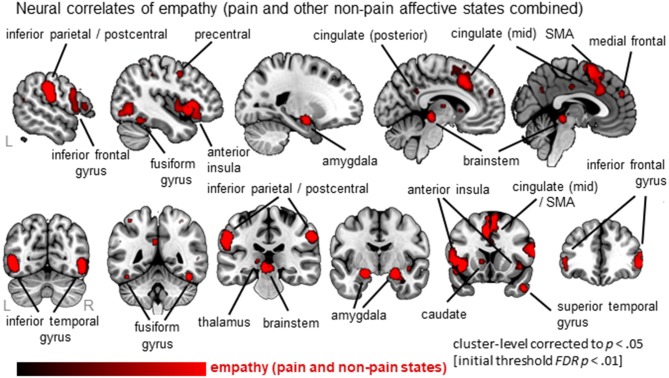
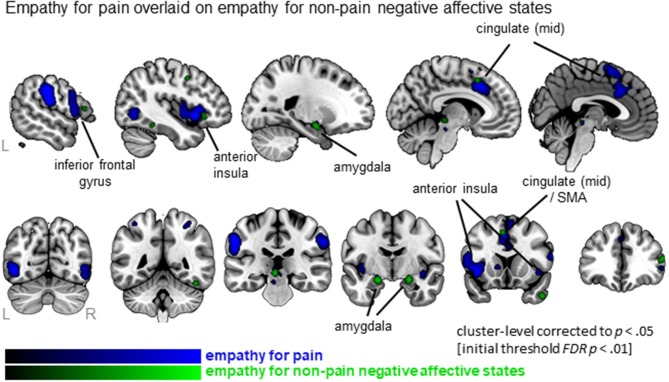
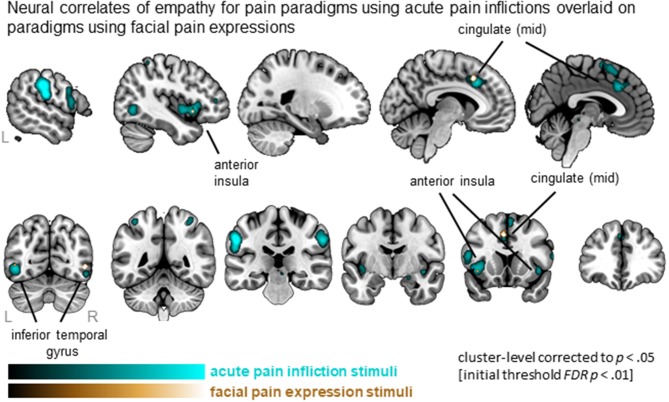
Empathy is an essential component of our social lives, allowing us to understand and share other people's affective and sensory states, including pain. Evidence suggests a core neural network-including anterior insula (AI) and mid-cingulate cortex (MCC)-is involved in empathy for pain. However, a similar network is associated to empathy for non-pain affective states, raising the question whether empathy for pain is unique in its neural correlates. Furthermore, it is yet unclear whether neural correlates converge across different stimuli and paradigms that evoke pain-empathy. We performed a coordinate-based activation likelihood estimation (ALE) meta-analysis to identify neural correlates of empathy, assess commonalities and differences between empathy for pain and for non-pain negative affective states, and differences between pain-empathy evoking stimuli (i.e., facial pain expressions vs. acute pain inflictions) and paradigms (i.e., perceptual/affective vs. cognitive/evaluative paradigms). Following a systematic search, data from 128 functional brain imaging studies presenting whole-brain results of an empathy condition vs. baseline/neutral condition were extracted. Synthesizing neural correlates of empathy confirmed a core network comprising AI, MCC, postcentral gyrus, inferior parietal lobe, thalamus, amygdala, and brainstem. There was considerable overlap in networks for empathy for pain and empathy for non-pain negative affective states. Important differences also arose: empathy for pain uniquely activated bilateral mid-insula and more extensive MCC. Regarding stimuli, painful faces and acute pain inflictions both evoked the core empathy regions, although acute pain inflictions activated additional regions including medial frontal and parietal cortex. Regarding paradigms, both perceptual/affective and cognitive/evaluative paradigms recruited similar neural circuitry, although cognitive/evaluative paradigms activated more left MCC regions while perceptual/affective paradigms activated more right AI. Taken together, our findings reveal that empathy for pain and empathy for non-pain negative affective states share considerable neural correlates, particularly in core empathy regions AI and MCC. Beyond these regions, important differences emerged, limiting generalizability of findings across different affective/sensory states. Within pain-empathy studies, the core regions were recruited robustly irrespective of stimuli or instructions, allowing one to tailor designs according to specific needs to some extent, while ensuring activation of core regions.
同理心是我们社会生活的重要组成部分,使我们能够理解并共享他人的情感和感觉状态,包括疼痛。有证据表明,一个核心神经网络——包括前脑岛(AI)和扣带中央回(MCC)——参与了对疼痛的同理心。然而,一个类似的网络与对非疼痛情感状态的同理心有关,这就提出了一个问题,即对疼痛的同理心在其神经关联方面是否独特。此外,尚不清楚不同刺激和引发疼痛同理心的范式之间的神经关联是否趋同。我们进行了一项基于坐标的激活可能性估计(ALE)元分析,以确定同理心的神经关联,评估对疼痛的同理心与对非疼痛负面情感状态的同理心之间的共性和差异,以及引发疼痛同理心的刺激(即面部疼痛表情与急性疼痛施加)和范式(即感知/情感与认知/评价范式)之间的差异。经过系统搜索,我们提取了128项功能性脑成像研究的数据,这些研究展示了同理心条件与基线/中性条件对比的全脑结果。对同理心神经关联的综合分析证实了一个核心网络,包括AI、MCC、中央后回、顶下小叶、丘脑、杏仁核和脑干。对疼痛的同理心和对非疼痛负面情感状态的同理心在网络上有相当大的重叠。也出现了重要差异:对疼痛的同理心独特地激活了双侧脑岛中部和更广泛的MCC。关于刺激,痛苦的面部表情和急性疼痛施加都引发了核心同理心区域,尽管急性疼痛施加激活了包括内侧额叶和顶叶皮质在内的其他区域。关于范式,感知/情感范式和认知/评价范式都招募了类似的神经回路,尽管认知/评价范式激活了更多左侧MCC区域,而感知/情感范式激活了更多右侧AI。综上所述,我们的研究结果表明,对疼痛的同理心和对非疼痛负面情感状态的同理心有相当多的神经关联,特别是在核心同理心区域AI和MCC。在这些区域之外,出现了重要差异,限制了研究结果在不同情感/感觉状态下的普遍性。在疼痛同理心研究中,无论刺激或指令如何,核心区域都会被强烈激活,这使得人们能够在一定程度上根据特定需求调整设计,同时确保核心区域的激活。