Instituto do Cancer do Estado de São Paulo, Faculdade de Medicina da Universidade de São Paulo, Av Dr Arnaldo, 251, São Paulo, ZIP code: 01246-000, Brazil.
São Paulo Clínicas Liver Cancer Group, Instituto do Câncer do Estado de São Paulo - Hospital das Clínicas Complex, Department of Gastroenterology, University of São Paulo School of Medicine, São Paulo, Brazil.
BMC Cancer. 2018 Dec 13;18(1):1250. doi: 10.1186/s12885-018-5173-0.
Before the targeted therapies era, cytotoxic chemotherapy (CCT) was an option for advanced hepatocellular carcinoma (HCC), even with the lack of supporting evidence. Since the last decade, sorafenib has been established as the first-line therapy. Although new agents are being incorporated, CCT is still considered in regions where new drugs are not available or for patients who progressed through the approved therapies and remain in good clinical condition. We aimed to describe our experience regarding the use of CCT as second-line treatment after sorafenib.
A database of 273 patients was evaluated. Patients that received CCT after sorafenib progression were selected for the analysis. Descriptive statistics was used for categorical and continue variables. Median survival was estimated with Kaplan-Meier curves. Variables were found to be significant if the two-sided p value was ≤ 0.05 on multivariate testing using the Cox regression model.
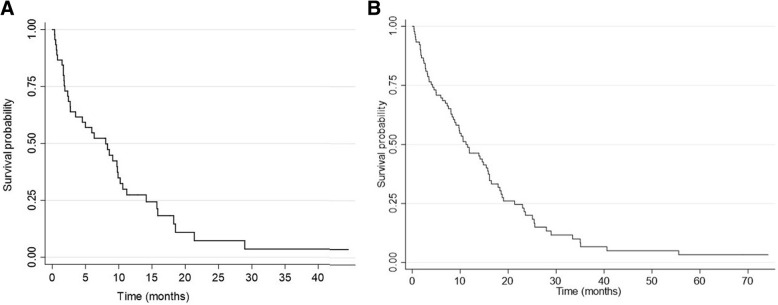
Forty-five patients received CCT; 33 (73.3%) had Child-Pugh classification A, and 34 (75.6%) had stage C according to the Barcelona Clinic Liver Cancer (BCLC) staging system. The most used regimen was doxorubicin in 25 patients (55.6%). Median overall survival (OS) was 8.05 months (95% confidence interval [CI] 2.73 - 9.88 months). The 6-month and 1-year survival probability was 52.4% and 27.36%, respectively. Eastern Cooperative Oncology Group performance status (ECOG PS) 0-1 and disease control with sorafenib was independently associated with better OS in patients treated with CCT. Any-grade toxicities were observed in 82.2% and grade 3-4 in 44.4% of the patients.
In accordance with previous studies, CCT had a notable rate of adverse events. The poor prognosis of this cohort suggests that CCT may not alter the natural history of HCC after sorafenib progression.
在靶向治疗时代之前,细胞毒化疗(CCT)是晚期肝细胞癌(HCC)的一种选择,尽管缺乏支持证据。自过去十年以来,索拉非尼已被确立为一线治疗药物。尽管新药物正在被纳入,但在新药不可用或在已通过批准的治疗方法进展且仍处于良好临床状况的患者中,仍考虑使用 CCT。我们旨在描述我们在索拉非尼进展后使用 CCT 作为二线治疗的经验。
评估了 273 例患者的数据库。选择接受索拉非尼进展后 CCT 的患者进行分析。使用描述性统计数据对分类和连续变量进行分析。使用 Kaplan-Meier 曲线估计中位生存期。如果多变量测试中双侧 p 值≤0.05,则认为变量具有统计学意义,使用 Cox 回归模型进行测试。
45 例患者接受 CCT;33 例(73.3%)患者Child-Pugh 分级为 A,34 例(75.6%)患者巴塞罗那临床肝癌(BCLC)分期为 C 期。最常用的方案是 25 例患者使用多柔比星(55.6%)。中位总生存期(OS)为 8.05 个月(95%置信区间[CI]为 2.73-9.88 个月)。6 个月和 1 年的生存率分别为 52.4%和 27.36%。ECOG PS 0-1 和索拉非尼的疾病控制与 CCT 治疗患者的更好 OS 独立相关。82.2%的患者出现任何级别的毒性,44.4%的患者出现 3-4 级毒性。
与先前的研究一致,CCT 的不良反应发生率较高。该队列的预后较差表明,CCT 可能不会改变索拉非尼进展后 HCC 的自然病程。