Soslow Robert A, Tornos Carmen, Park Kay J, Malpica Anais, Matias-Guiu Xavier, Oliva Esther, Parkash Vinita, Carlson Joseph, McCluggage W Glenn, Gilks C Blake
Department of Pathology, Memorial Sloan Kettering Cancer Center, New York (R.A.S, K.J.P.) Department of Pathology, Stony Brook Hospital, SUNY, Stony Brook (C.T.), New York Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, Texas (A.M.) Pathology Department, University Hospital Arnau de Vilanova and University Hospital of Bellvitge, Biomedical Research Institute, and Bellvitge Biomedical Institute, University of Lleida, CIBERONC, Spain (X.M.-G.) Department of Pathology, Massachusetts General Hospital, Boston, Massachusetts (E.O.) Department of Pathology, Yale School of Medicine and the Yale School of Public Health, New Haven, Connecticut (V.P.) Department of Oncology-Pathology, Karolinska Institutet and Department of Pathology and Cytology, Karolinska University Hospital, Stockholm, Sweden (J.C.) Department of Pathology, Belfast Health and Social Care Trust, Belfast, UK (W.G.M.) Department of Pathology and Laboratory Medicine, Vancouver General Hospital and University of British Columbia, Vancouver, BC, Canada (C.B.G.).
Int J Gynecol Pathol. 2019 Jan;38 Suppl 1(Iss 1 Suppl 1):S64-S74. doi: 10.1097/PGP.0000000000000518.
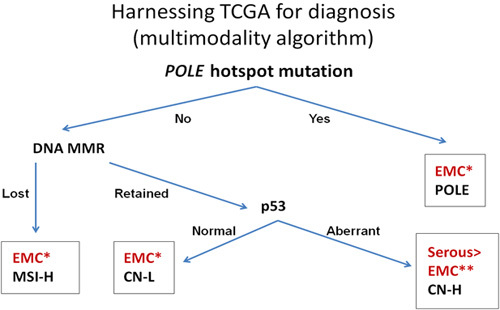
In this review, we sought to address 2 important issues in the diagnosis of endometrial carcinoma: how to grade endometrial endometrioid carcinomas and how to incorporate the 4 genomic subcategories of endometrial carcinoma, as identified through The Cancer Genome Atlas, into clinical practice. The current International Federation of Gynecology and Obstetrics grading scheme provides prognostic information that can be used to guide the extent of surgery and use of adjuvant chemotherapy or radiation therapy. We recommend moving toward a binary scheme to grade endometrial endometrioid carcinomas by considering International Federation of Gynecology and Obstetrics defined grades 1 and 2 tumors as "low grade" and grade 3 tumors as "high grade." The current evidence base does not support the use of a 3-tiered grading system, although this is considered standard by International Federation of Gynecology and Obstetrics, the American College of Obstetricians and Gynecologists, and the College of American Pathologists. As for the 4 genomic subtypes of endometrial carcinoma (copy number low/p53 wild-type, copy number high/p53 abnormal, polymerase E mutant, and mismatch repair deficient), which only recently have been identified, there is accumulating evidence showing these categories can be reproducibly diagnosed and accurately assessed based on biopsy/curettage specimens as well as hysterectomy specimens. Furthermore, this subclassification system can be adapted for current clinical practice and is of prognostic significance independent of conventional variables used for risk assessment in patients with endometrial carcinoma (eg, stage). It is too soon to recommend the routine use of genomic classification in this setting; however, with further evidence, this system may become the basis for the subclassification of all endometrial carcinomas, supplanting (partially or completely) histotype, and grade. These recommendations were developed from the International Society of Gynecological Pathologists Endometrial Carcinoma project.
在本综述中,我们试图解决子宫内膜癌诊断中的两个重要问题:如何对子宫内膜样腺癌进行分级,以及如何将通过癌症基因组图谱鉴定出的子宫内膜癌的4种基因组亚类纳入临床实践。目前的国际妇产科联盟(International Federation of Gynecology and Obstetrics,FIGO)分级方案提供了预后信息,可用于指导手术范围以及辅助化疗或放疗的使用。我们建议采用二元分级方案,将FIGO定义的1级和2级肿瘤视为“低级别”,3级肿瘤视为“高级别”,以此对子宫内膜样腺癌进行分级。尽管FIGO、美国妇产科医师学会(American College of Obstetricians and Gynecologists)和美国病理学家学会(College of American Pathologists)认为三级分级系统是标准的,但目前的证据基础并不支持使用该系统。至于最近才被鉴定出的子宫内膜癌的4种基因组亚型(拷贝数低/p53野生型、拷贝数高/p53异常、聚合酶E突变型和错配修复缺陷型),越来越多的证据表明,基于活检/刮宫标本以及子宫切除标本,这些类别能够被重复性诊断并准确评估。此外,这种亚分类系统可适用于当前的临床实践,并且独立于用于评估子宫内膜癌患者风险的传统变量(如分期)具有预后意义。在这种情况下,现在就推荐常规使用基因组分类还为时过早;然而,随着更多证据的出现,该系统可能会成为所有子宫内膜癌亚分类的基础,(部分或完全)取代组织学类型和分级。这些建议是由国际妇科病理学家学会子宫内膜癌项目制定的。