Lorenzetti Diane L, Quan Hude, Lucyk Kelsey, Cunningham Ceara, Hennessy Deirdre, Jiang Jason, Beck Cynthia A
Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, 3330 Hospital Drive NW, Calgary, AB, T2N4N1, Canada.
Department of Psychiatry, Cumming School of Medicine, University of Calgary, 3330 Hospital Drive NW, Calgary, AB, T2N4N1, Canada.
BMC Emerg Med. 2018 Oct 25;18(1):36. doi: 10.1186/s12873-018-0188-z.
Physician chart documentation can facilitate patient care decisions, reduce treatment errors, and inform health system planning and resource allocation activities. Although accurate and complete patient chart data supports quality and continuity of patient care, physician documentation often varies in terms of timeliness, legibility, clarity and completeness. While many educational and other approaches have been implemented in hospital settings, the extent to which these interventions can improve the quality of documentation in emergency departments (EDs) is unknown.
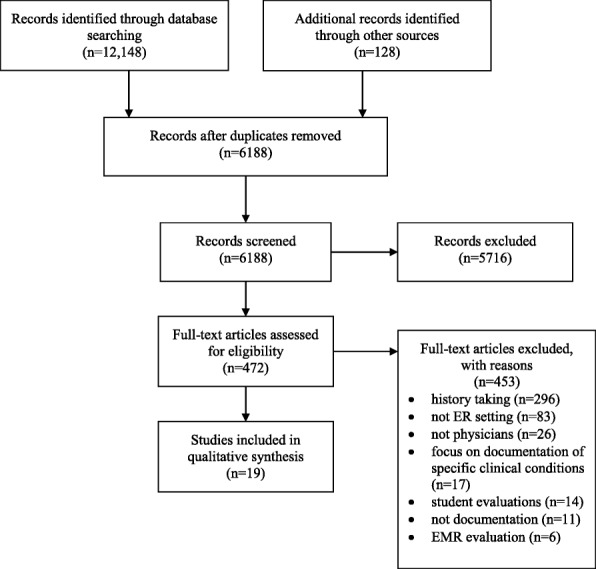
We conducted a systematic review to assess the effectiveness of approaches to improve ED physician documentation. Peer reviewed electronic databases, grey literature sources, and reference lists of included studies were searched to March 2015. Studies were included if they reported on outcomes associated with interventions designed to enhance the quality of physician documentation.
Nineteen studies were identified that report on the effectiveness of interventions to improve physician documentation in EDs. Interventions included audit/feedback, dictation, education, facilitation, reminders, templates, and multi-interventions. While ten studies found that audit/feedback, dictation, pharmacist facilitation, reminders, templates, and multi-pronged approaches did improve the quality of physician documentation across multiple outcome measures, the remaining nine studies reported mixed results.
Promising approaches to improving physician documentation in emergency department settings include audit/feedback, reminders, templates, and multi-pronged education interventions. Future research should focus on exploring the impact of implementing these interventions in EDs with and without emergency medical record systems (EMRs), and investigating the potential of emerging technologies, including EMR-based machine-learning, to promote improvements in the quality of ED documentation.
医生病历记录有助于做出患者护理决策、减少治疗错误,并为卫生系统规划和资源分配活动提供信息。尽管准确完整的患者病历数据有助于保障患者护理的质量和连续性,但医生记录在及时性、易读性、清晰度和完整性方面往往存在差异。虽然医院环境中已经实施了许多教育和其他方法,但这些干预措施能在多大程度上提高急诊科(ED)的记录质量尚不清楚。
我们进行了一项系统评价,以评估改善急诊科医生记录的方法的有效性。检索了经过同行评审的电子数据库、灰色文献来源以及纳入研究的参考文献列表,检索截至2015年3月。如果研究报告了与旨在提高医生记录质量的干预措施相关的结果,则纳入该研究。
共确定了19项报告急诊科医生记录干预措施有效性的研究。干预措施包括审核/反馈、听写、教育、协助、提醒、模板和多种干预措施。虽然10项研究发现审核/反馈、听写、药剂师协助、提醒、模板和多管齐下的方法确实在多个结果指标上提高了医生记录的质量,但其余9项研究报告的结果不一。
在急诊科环境中,改善医生记录的有前景的方法包括审核/反馈、提醒、模板和多管齐下的教育干预措施。未来的研究应侧重于探索在有和没有急诊医疗记录系统(EMR)的急诊科实施这些干预措施的影响,并研究包括基于EMR的机器学习在内的新兴技术促进急诊科记录质量提高的潜力。