McManus Kathleen A, Rhodes Anne, Yerkes Lauren, Engelhard Carolyn L, Ingersoll Karen S, Dillingham Rebecca
Division of Infectious Diseases and International Health, University of Virginia, Charlottesville, Virginia.
Center for Health Policy, University of Virginia, Charlottesville, Virginia.
Open Forum Infect Dis. 2018 Oct 31;5(12):ofy283. doi: 10.1093/ofid/ofy283. eCollection 2018 Dec.
For year 1 of the Affordable Care Act (ACA), Virginia AIDS Drug Assistance Program (ADAP) clients with Qualified Health Plans (QHPs) achieved a higher rate of viral suppression. This study characterizes the demographic and health care delivery factors associated with QHP enrollment in year 2 and assesses the relationship between 2015 QHP coverage and HIV viral suppression.
The cohort included Virginia ADAP clients who were eligible for ADAP-funded QHPs. Data were collected from 2014 to 2015. Multivariable binary logistic regression was conducted to assess the association of demographic and health care delivery factors with QHP enrollment and viral suppression.
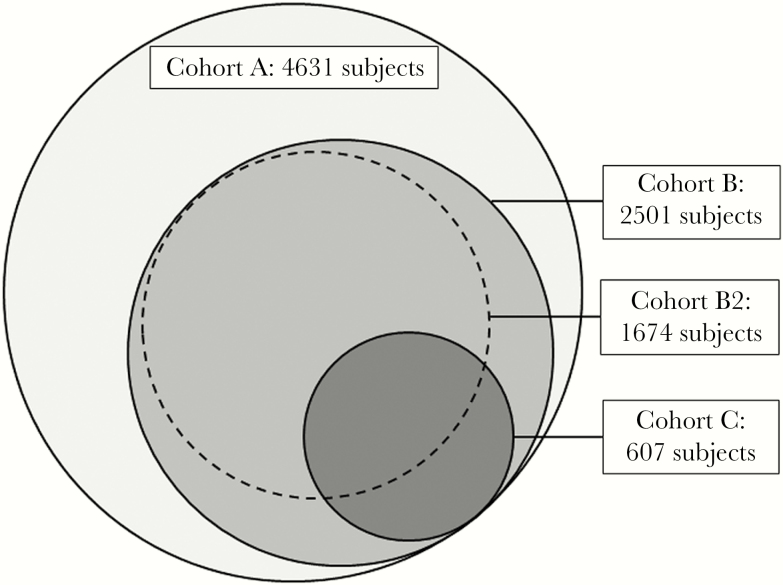
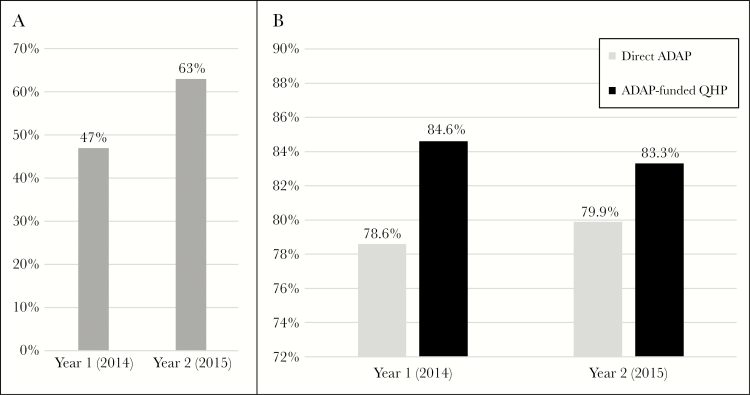
In year 2, 63% of the cohort (n = 4631) enrolled in QHPs; 2015 ADAP-funded QHP enrollment was associated with 2014 ADAP-funded QHP (adjusted odds ratio [aOR], 111.11; 95% confidence interval [CI], 90.91-166.67), 2014 engagement in care (aOR, 2.16; 95% CI, 1.65-2.82), age ( < .001), race/ethnicity ( = .03), financial status ( < .001), and region ( < .001). For clients engaged in care (n = 2501), viral suppression was higher (83.3%) for those with ADAP-funded QHP coverage than for those who received medications from ADAP (79.9%). In multivariable binary logistic regression, achieving viral suppression was associated with 2015 QHP coverage (aOR, 1.27; 95% CI, 1.01-1.60), an initially undetectable viral load (aOR, 2.69; 95% CI, 2.13-3.39), gender ( = .03), age ( = .01), no AIDS diagnosis (aOR, 1.41; 95% CI, 1.12-1.78), financial status ( = .004), and region ( < .001).
Virginia ADAP client 2015 QHP enrollment increased compared with year 1 and varied based on demographic and health care delivery factors. QHP coverage was again associated with viral suppression, an essential outcome for individuals and for public health.
在《平价医疗法案》(ACA)实施的第一年,弗吉尼亚艾滋病药物援助计划(ADAP)的客户通过合格健康计划(QHP)实现了更高的病毒抑制率。本研究描述了与第二年QHP参保相关的人口统计学和医疗服务提供因素,并评估了2015年QHP覆盖与HIV病毒抑制之间的关系。
该队列包括有资格获得ADAP资助的QHP的弗吉尼亚ADAP客户。数据收集于2014年至2015年。进行多变量二元逻辑回归以评估人口统计学和医疗服务提供因素与QHP参保及病毒抑制之间的关联。
在第二年,该队列中有63%(n = 4631)的人参保了QHP;2015年ADAP资助的QHP参保与2014年ADAP资助的QHP(调整优势比[aOR],111.11;95%置信区间[CI],90.91 - 166.67)、2014年接受治疗(aOR,2.16;95% CI,1.65 - 2.82)、年龄(< 0.001)、种族/族裔(= 0.03)、财务状况(< 0.001)和地区(< 0.001)相关。对于接受治疗的客户(n = 2501),有ADAP资助的QHP覆盖的客户的病毒抑制率更高(83.3%),高于那些从ADAP获得药物的客户(79.9%)。在多变量二元逻辑回归中,实现病毒抑制与2015年QHP覆盖(aOR,1.27;95% CI,1.01 - 1.60)、最初病毒载量不可检测(aOR,2.69;95% CI,2.13 - 3.39)、性别(= 0.03)、年龄(= 0.01)、无艾滋病诊断(aOR,1.41;95% CI,1.12 - 1.78)、财务状况(= 0.004)和地区(< 0.001)相关。
与第一年相比,弗吉尼亚ADAP客户在2015年的QHP参保有所增加,且因人口统计学和医疗服务提供因素而异。QHP覆盖再次与病毒抑制相关,这对个人和公共卫生都是一项重要成果。