Yang Dennis, Samarasena Jason B, Jamil Laith H, Chang Kenneth J, Lee David, Ona Mel A, Lo Simon K, Gaddam Srinivas, Liu Quin, Draganov Peter V
Division of Gastroenterology and Hepatology, University of Florida, Gainesville, Florida, United States.
Division of Gastroenterology and Hepatology, University of California Irvine, Irvine, California, United States.
Endosc Int Open. 2018 Dec;6(12):E1423-E1430. doi: 10.1055/a-0770-2700. Epub 2018 Dec 5.
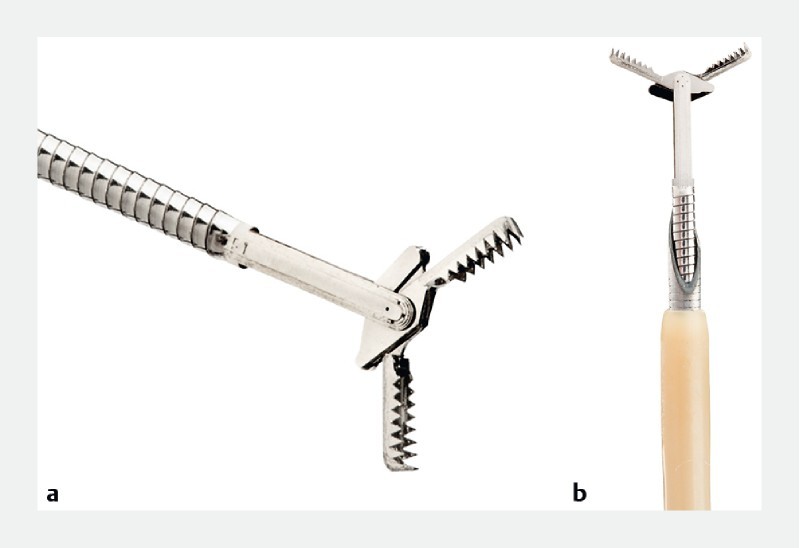
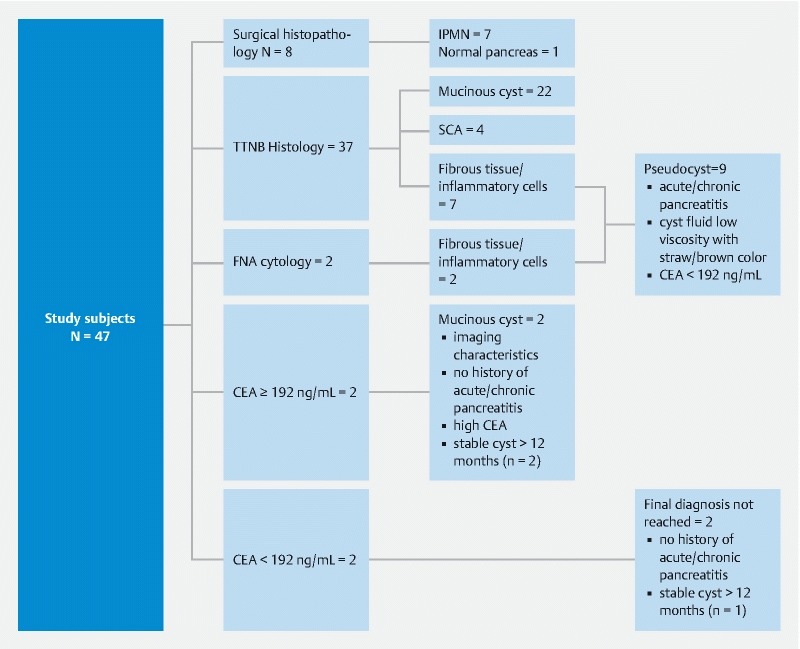
Accurate diagnosis and classification of pancreatic cysts (PCs) remains a challenge. The aims of this study were to: (1) evaluate the safety and technical success of a novel microforceps for EUS-guided through-the-needle biopsy (TTNB) of PCs; and (2) assess its diagnostic yield for mucinous PCs when compared to FNA cyst fluid analysis and cytology. This was a multicenter retrospective analysis of 47 patients who underwent EUS-FNA and TTNB for PCs between January 2014 and June 2017. Technical success was defined as acquisition of a specimen adequate for cytologic or histological evaluation. Cyst fluid carcinoembryonic antigen (CEA) was used to initially categorize cysts as non-mucinous (CEA < 192 ng/mL) or mucinous (CEA ≥ 192 ng/mL). Final diagnosis was based on identifiable mucinous pancreatic cystic epithelium on cytology, microforceps histology and/or surgical histology when available. Forty-seven patients with PCs (mean size 30.7 mm) were included. TTNB was successfully performed in 46 of 47 (97.9 %). Technical success was significantly lower with FNA (48.9 %) compared to TTNB (85.1 %) ( < .001). For cysts with insufficient amount of fluid for CEA (n = 19) or CEA < 192 ng/mL, the cumulative incremental diagnostic yield of a mucinous PC was significantly higher with TTNB vs. FNA (52.6 % vs 18.4 %; = .004). TTNB alone (34.4 %) diagnosed more mucinous PCs than either CEA ≥ 192 ng/mL alone (6.3 %) or when combined with FNA cytology (9.4 %). One episode of self-limited bleeding (2.1 %) and one of pancreatitis (2.1 %) occurred. EUS-TTNB is safe and effective for evaluating PCs. TTNB may help increase the diagnostic yield of mucinous PCs.
胰腺囊肿(PCs)的准确诊断和分类仍然是一项挑战。本研究的目的是:(1)评估一种新型微型活检钳用于内镜超声引导下经针穿刺活检(TTNB)诊断PCs的安全性和技术成功率;(2)与细针穿刺抽吸(FNA)囊肿液分析及细胞学检查相比,评估其对黏液性PCs的诊断率。这是一项对2014年1月至2017年6月期间接受内镜超声引导下细针穿刺抽吸和经针穿刺活检诊断PCs的47例患者进行的多中心回顾性分析。技术成功定义为获取到足以进行细胞学或组织学评估的标本。囊肿液癌胚抗原(CEA)最初用于将囊肿分类为非黏液性(CEA<192 ng/mL)或黏液性(CEA≥192 ng/mL)。最终诊断基于细胞学、微型活检钳组织学检查及(如有)手术组织学检查中可识别的黏液性胰腺囊性上皮。纳入了47例PCs患者(平均大小30.7 mm)。47例患者中有46例(97.9%)成功进行了TTNB。与TTNB(85.1%)相比,FNA的技术成功率(48.9%)显著更低(P<0.001)。对于囊肿液量不足以检测CEA的囊肿(n = 19)或CEA<192 ng/mL的囊肿,TTNB诊断黏液性PCs的累积增量诊断率显著高于FNA(52.6%对18.4%;P = 0.004)。单独TTNB(34.4%)诊断出的黏液性PCs比单独CEA≥192 ng/mL(6.3%)或与FNA细胞学检查联合时(9.4%)更多。发生了1例自限性出血(2.1%)和1例胰腺炎(2.1%)。内镜超声引导下经针穿刺活检对于评估PCs是安全有效的。TTNB可能有助于提高黏液性PCs的诊断率。