Pace Romina, Rahme Elham, Da Costa Deborah, Dasgupta Kaberi
Centre for Outcomes Research and Evaluation, Research Institute of the McGill University Health Centre, Montreal, QC, Canada,
Department of Medicine, McGill University Health Center, Montreal, QC, Canada,
Clin Epidemiol. 2018 Dec 3;10:1827-1838. doi: 10.2147/CLEP.S184319. eCollection 2018.
The aim of this study was to examine the association between gestational diabetes mellitus (GDM) and depression incidence in mothers and fathers during prenatal and postnatal periods.
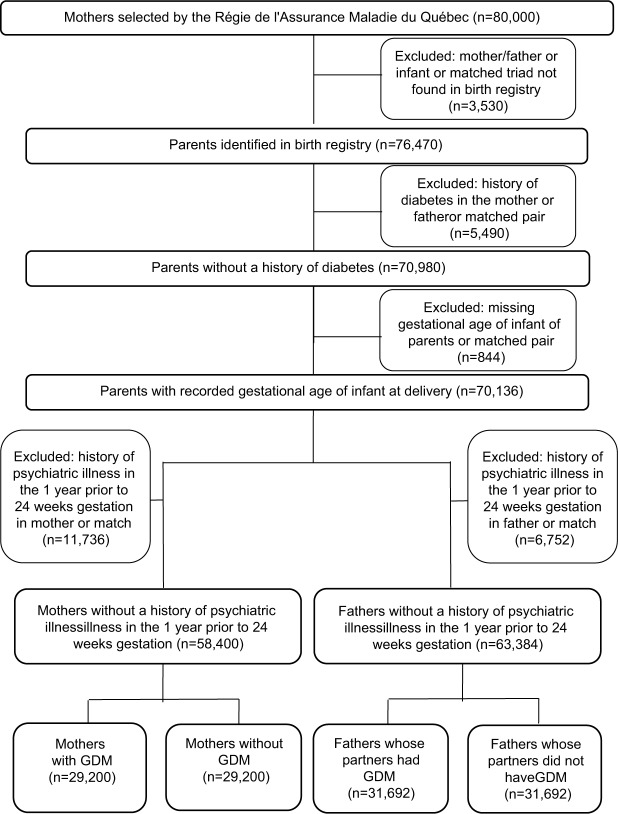
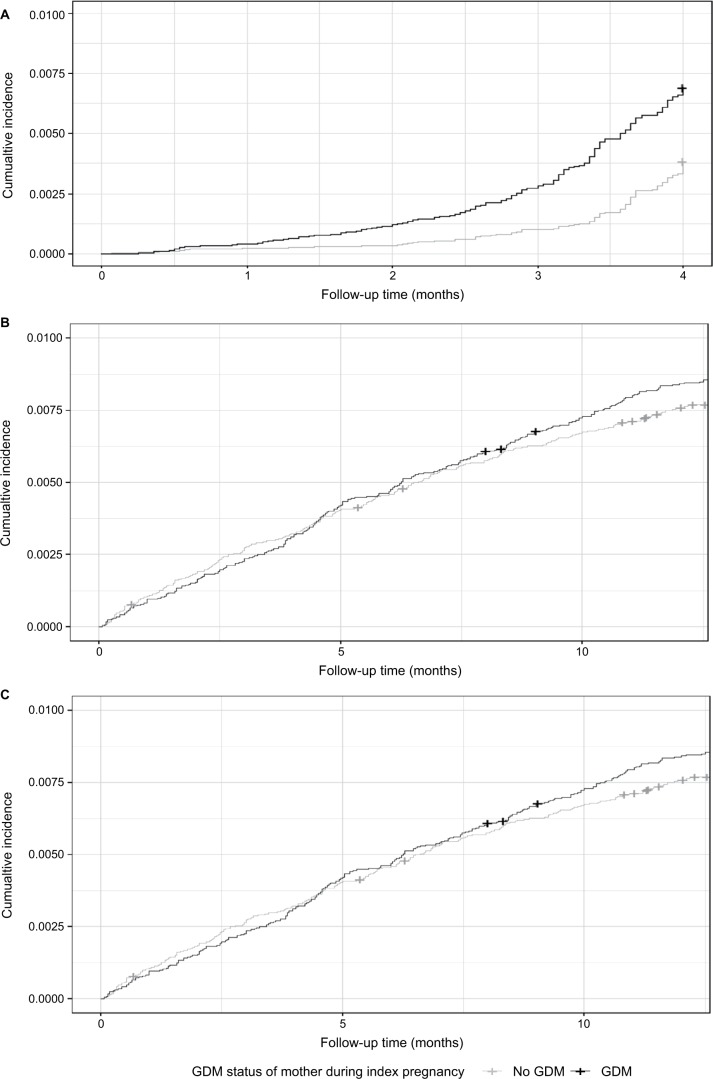
Matched pairs (GDM vs no GDM) of randomly selected mothers with singleton live births (matched by age group, delivery year, and health region) and their partners (Quebec, Canada; cohort inception 1990-2007) were assessed for a composite outcome of depression/self-harm/suicide using a health administrative database. We examined the association of GDM and the composite outcome in the following three nonoverlapping periods: 1) 24 weeks gestation up to delivery; 2) delivery up to 1 year postpartum; and 3) 1 year postpartum to study end (March 31, 2012). We used stratified Cox proportional regression hazards models, with three models in mothers and three models in fathers, corresponding to each of the time periods of interest.
In the 58,400 mothers, women with GDM had a nearly twofold greater risk (adjusted HR: 1.82, 95% CI 1.28, 2.59) of being diagnosed with depression compared to those without GDM during the prenatal period. In the first year postpartum, there was no conclusive difference observed between the two groups of mothers (adjusted HR: 1.05, 95% CI 0.84, 1.30). Beyond the first year postpartum, there was an 8% increased risk (adjusted HR: 1.08, 95% CI 1.03, 1.14) of depression in women with a history GDM compared to those without. A total of 63,384 fathers were included in our analyses, and no association between GDM in one's partner and depression was found during any of the three time periods evaluated.
GDM is associated with an increased risk of depression in women particularly during pregnancy highlighting the need to screen for depression and provide supportive interventions during this period.
本研究旨在探讨妊娠期糖尿病(GDM)与父母在产前和产后抑郁症发病率之间的关联。
采用健康管理数据库,对随机选取的单胎活产母亲(按年龄组、分娩年份和健康区域匹配)及其伴侣(加拿大魁北克;队列起始于1990 - 2007年)进行配对(GDM组与非GDM组),评估抑郁/自我伤害/自杀的综合结局。我们在以下三个不重叠的时间段内研究GDM与综合结局的关联:1)妊娠24周直至分娩;2)分娩至产后1年;3)产后1年至研究结束(2012年3月31日)。我们使用分层Cox比例回归风险模型,母亲和父亲各有三个模型,分别对应每个感兴趣的时间段。
在58400名母亲中,患有GDM的女性在孕期被诊断为抑郁症的风险几乎是非GDM女性的两倍(调整后风险比:1.82,95%置信区间1.28,2.59)。在产后第一年,两组母亲之间未观察到确凿差异(调整后风险比:1.05,95%置信区间0.84,1.30)。产后一年以后,有GDM病史的女性患抑郁症的风险比无GDM病史的女性增加8%(调整后风险比:1.08,95%置信区间1.03,1.14)。我们的分析共纳入63384名父亲,在评估的三个时间段中的任何一个时间段内,均未发现伴侣患有GDM与父亲患抑郁症之间存在关联。
GDM与女性患抑郁症的风险增加有关,尤其是在孕期,这凸显了在此期间筛查抑郁症并提供支持性干预措施的必要性。