Puthoff Teresa D, Shah Hevil, Slaughter Jonathan L, Bapat Roopali
Department of Pharmacy Services, Nationwide Children's Hospital.
Department of Pediatrics, Nationwide Children's Hospital.
Pediatr Qual Saf. 2018 Sep 28;3(5):e106. doi: 10.1097/pq9.0000000000000106. eCollection 2018 Sep-Oct.
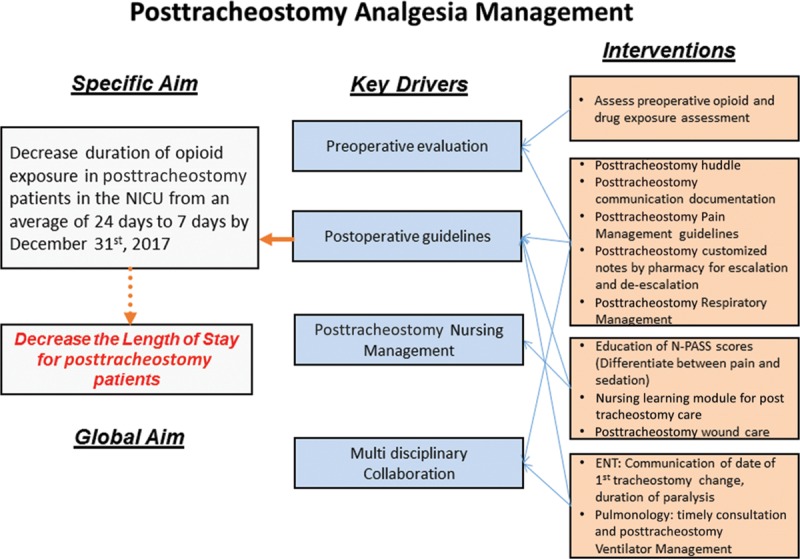
As survival has improved in the Neonatal Intensive Care Unit (NICU), there has been a 10-fold increase in the proportion of infants requiring a tracheostomy. At our institution, we observed a wide variation in the duration of opioid use posttracheostomy from 6 to 148 days. We aimed to decrease the duration of opioid exposure in postoperative tracheostomy patients in the NICU from a baseline average of 24 days to 7 days by December 31, 2017.
We established a multidisciplinary team to develop change ideas to implement in 3 Plan-Do-Study-Act cycles that focused on enhanced care plan standardization and communication in patient care rounds with subsequent documentation in the medical record and the timely addition of dexmedetomidine to the postoperative care plan.
Baseline population was from October 2014 to December 2016. The mean posttracheostomy opioid duration was 24.6 days (range, 6-148 days); neuromuscular blockade was 2.89 days (range, 0-9 days), and benzodiazepine exposure was 20.9 days (range, 1-114 days). Following our interventions, the mean duration of posttracheostomy opioid duration was 5.4 days (range, 4-21 days); neuromuscular blockade was 3.14 days (range, 1-5 days), benzodiazepine duration was 8.88 days (range, 4-25 days), and dexmedetomidine was 4.6 days (range, 0-32 days).
We utilized quality improvement methodology to standardize posttracheostomy management and demonstrate that we could significantly reduce the duration of opioid and benzodiazepine use after tracheostomy with the timely addition of dexmedetomidine, a structured written daily care plan, and clarification of roles and responsibilities.
随着新生儿重症监护病房(NICU)中婴儿存活率的提高,需要进行气管造口术的婴儿比例增加了10倍。在我们机构,我们观察到气管造口术后使用阿片类药物的持续时间差异很大,从6天到148天不等。我们的目标是到2017年12月31日,将NICU中气管造口术后患者的阿片类药物暴露持续时间从基线平均24天减少到7天。
我们成立了一个多学科团队,以制定变革想法,并在3个计划-执行-研究-行动周期中实施,这些周期侧重于加强护理计划标准化以及在患者护理查房中的沟通,随后在病历中记录,并及时将右美托咪定添加到术后护理计划中。
基线人群为2014年10月至2016年12月。气管造口术后阿片类药物的平均持续时间为24.6天(范围为6 - 148天);神经肌肉阻滞为2.89天(范围为0 - 9天),苯二氮䓬类药物暴露为20.9天(范围为1 - 114天)。在我们的干预措施实施后,气管造口术后阿片类药物的平均持续时间为5.4天(范围为4 - 21天);神经肌肉阻滞为3.14天(范围为1 - 5天),苯二氮䓬类药物持续时间为8.88天(范围为4 - 25天),右美托咪定持续时间为4.6天(范围为0 - 32天)。
我们采用质量改进方法来规范气管造口术后管理,并证明通过及时添加右美托咪定、制定结构化的每日书面护理计划以及明确角色和职责,我们可以显著缩短气管造口术后阿片类药物和苯二氮䓬类药物的使用时间。