Murri Rita, Camici Marta, Posteraro Brunella, Giovannenze Francesca, Taccari Francesco, Ventura Giulio, Scoppettuolo Giancarlo, Sanguinetti Maurizio, Cauda Roberto, Fantoni Massimo
Institute of Infectious Diseases, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy,
Institute of Medical Pathology and Semeiotics, Fondazione Policlinico Universitario A. Gemelli IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy.
Infect Drug Resist. 2018 Dec 20;12:19-24. doi: 10.2147/IDR.S181489. eCollection 2019.
To assess the performance of the (1,3)-β-D-glucan (BDG) detection assay in a large cohort of patients with suspected candidemia who were admitted to non-intensive care unit hospital wards.
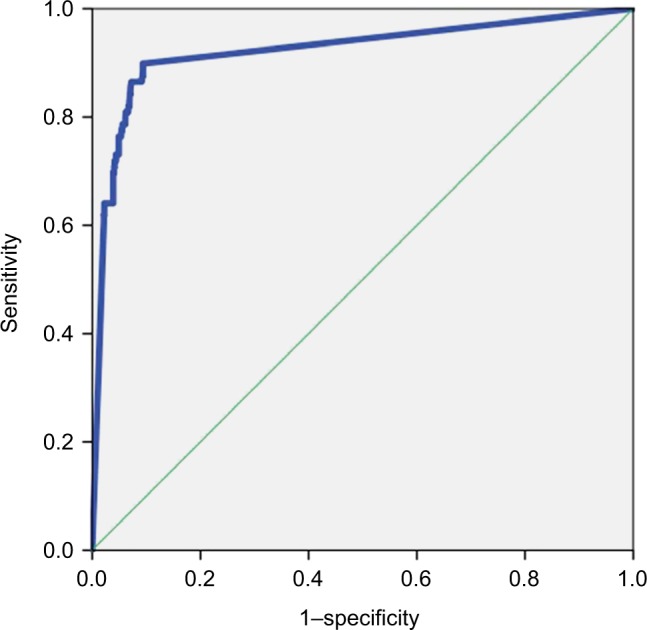
This observational, retrospective cohort study was conducted in a 1,100-bed university hospital in Rome, where an infectious disease consultation team has been operational. Two groups of patients were included in the analysis: Group 1, patients with bloodstream infection (BSI) who had at least one BDG test performed ±48 hours from the first positive blood culture ( BSI Group) and Group 2, patients with risk factors for candidemia who had at least one BDG test but had negative blood cultures (Control Group). Both Group 1 and Group 2 did not receive prior antifungal therapy. Different BDG cutoff values were considered: 80, 200, 300, 400, and ≥500 pg/mL. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and area under the receiver operating characteristic curve were calculated.
A total of 1,296 patients were studied. Of them, 100 patients (candidemic) were in Group 1 and the remaining 1,196 patients (controls) were in Group 2. There were no differences in demographic characteristics between patients of the two groups. According to the above cutoff values, sensitivity (%) and specificity (%) of the BDG assay ranged from 91 to 60.7 and 87.7 to 97.8, respectively, whereas the PPV (%) and NPV (%) ranged from 38.2 to 68.3 and 99.1 to 97.0, respectively.
Serum BDG has a very high NPV in a population witĥ10% prevalence of candidemia. This NPV may support decisions to discontinue antifungal therapy in those patients who were empirically treated because of the suspect of candidemia.
评估(1,3)-β-D-葡聚糖(BDG)检测法在一大批入住非重症监护病房的疑似念珠菌血症患者中的表现。
这项观察性、回顾性队列研究在罗马一家拥有1100张床位的大学医院进行,该医院有一个传染病会诊团队。分析纳入两组患者:第1组,血流感染(BSI)患者,在首次血培养阳性后±48小时至少进行了一次BDG检测(BSI组);第2组,有念珠菌血症危险因素且至少进行了一次BDG检测但血培养阴性的患者(对照组)。第1组和第2组患者均未接受过抗真菌治疗。考虑了不同的BDG临界值:80、200、300、400和≥500 pg/mL。计算了敏感性、特异性、阳性预测值(PPV)、阴性预测值(NPV)和受试者工作特征曲线下面积。
共研究了1296例患者。其中,第1组有100例(念珠菌血症患者),其余1196例患者(对照组)在第2组。两组患者的人口统计学特征无差异。根据上述临界值,BDG检测法的敏感性(%)和特异性(%)分别为91至60.7和87.7至97.8,而PPV(%)和NPV(%)分别为38.2至68.3和99.1至97.0。
在念珠菌血症患病率为10%的人群中,血清BDG具有非常高的NPV。该NPV可能有助于支持对因疑似念珠菌血症而接受经验性治疗的患者停止抗真菌治疗的决策。