Yao Ji-Jin, Zhang Fan, Zhang Guang-Shun, Deng Xiao-Wu, Zhang Wang-Jian, Lawrence Wayne R, Zou Lu, Zhang Xiao-Shi, Lu Li-Xia
Department of Radiation Oncology, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Sun Yat-Sen University Cancer Center, Guangzhou 510060, Guangdong Province, People's Republic of China,
Department of Radiation Oncology, The Fifth Affiliated Hospital of Sun Yat-Sen University, Zhuhai 519001, Guangdong Province, People's Republic of China.
Cancer Manag Res. 2018 Dec 14;10:6985-6996. doi: 10.2147/CMAR.S185017. eCollection 2018.
There still remains no well-established treatment strategy for head and neck mucosal melanoma (HNMM). We aim to evaluate the effectiveness and safety of primary surgery with postoperative radiotherapy for this disease.
A single-arm, Phase II clinical trial was conducted at Sun Yat-Sen University Cancer Center. Patients with nonmetastatic, histologically proven HNMM were prospectively enrolled. Patients received primary surgery followed by intensity-modulated radiotherapy with an equivalent dose at 2 Gy per fraction of 65-70 Gy to CTV1 (high-risk regions including tumor bed) and 50-55 Gy to CTV2 (low-risk regions). Additional use of adjuvant chemotherapy (AC) depended on consultation from a multidisciplinary team. This trial is registered with ClinicalTrials.gov, number NCT03138642.
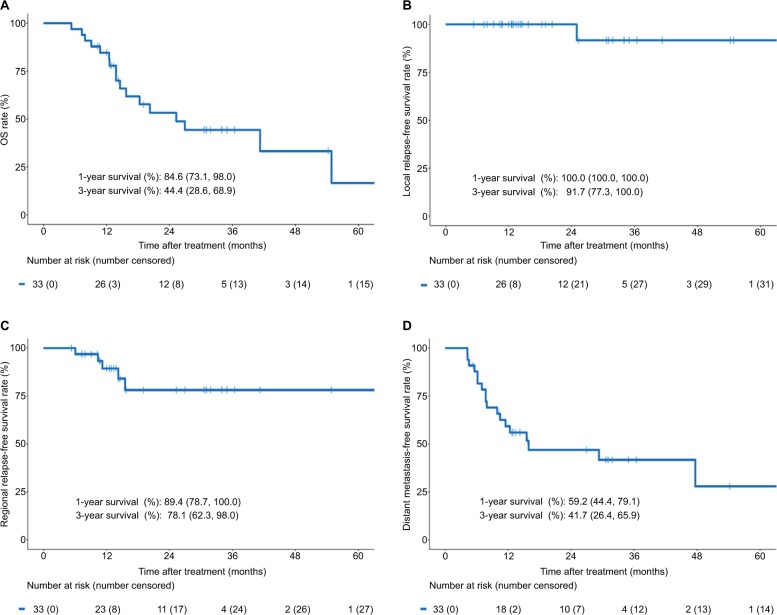
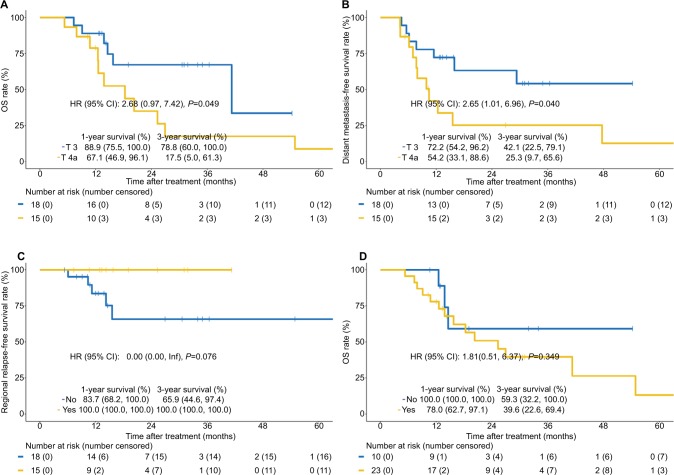
A total of 33 patients were enrolled and analyzed between July 2010 and November 2016. There were 18 (54.5%) patients with T3 disease and 15 (45.5%) patients with T4a disease. The median age at diagnosis was 58 years (range 27-83 years), and 61% of the cohort were males. The overall median follow-up duration was 25.3 months (range 5.3-67.1 months). The 3-year overall survival (OS), local relapse-free survival (LRFS), regional relapse-free survival (RRFS), and distant metastasis-free survival (DMFS) rates were 44.4, 91.7, 78.1, and 41.7%, respectively. Patients with T4a disease showed significantly inferior OS (=0.049) and DMFS (=0.040) than those with T3 disease. Prophylactic neck radiation (PNR) was nearly associated with superior RRFS (=0.078). However, there was no significant difference in OS, LRFS, RRFS, and DMFS for patients treated with or without AC (>0.05 for all). Toxicities were generally mild to moderate.
Primary surgery with postoperative radiotherapy yielded excellent local control and acceptable toxicity profile for HNMM. Nevertheless, high rates of distant metastases resulted in limited survival.
头颈部黏膜黑色素瘤(HNMM)仍没有成熟的治疗策略。我们旨在评估原发性手术联合术后放疗对该疾病的有效性和安全性。
在中山大学肿瘤防治中心开展了一项单臂II期临床试验。前瞻性纳入经组织学证实的非转移性HNMM患者。患者接受原发性手术,随后进行调强放疗,CTV1(包括瘤床的高风险区域)的等效剂量为每分次2 Gy,共65 - 70 Gy,CTV2(低风险区域)为50 - 55 Gy。辅助化疗(AC)的额外使用取决于多学科团队的会诊意见。本试验已在ClinicalTrials.gov注册,注册号为NCT03138642。
2010年7月至2016年11月期间共纳入33例患者并进行分析。有18例(54.5%)患者为T3期疾病,15例(45.5%)患者为T4a期疾病。诊断时的中位年龄为58岁(范围27 - 83岁),队列中61%为男性。总体中位随访时间为25.3个月(范围5.3 - 67.1个月)。3年总生存率(OS)、局部无复发生存率(LRFS)、区域无复发生存率(RRFS)和远处转移无复发生存率(DMFS)分别为44.4%、91.7%、78.1%和41.7%。T4a期疾病患者的OS(P = 0.049)和DMFS(P = 0.040)显著低于T3期疾病患者。预防性颈部放疗(PNR)与较高的RRFS近相关(P = 0.078)。然而,接受或未接受AC治疗的患者在OS、LRFS、RRFS和DMFS方面无显著差异(所有P均>0.05)。毒性反应一般为轻至中度。
原发性手术联合术后放疗对头颈部黏膜黑色素瘤产生了良好的局部控制效果且毒性反应可接受。尽管如此,远处转移率高导致生存率受限。