Sun Xiangrong, Jiang Guohui, Ju Xinyue, Fu Hongmei
Department of Neurology, the Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, China.
Medicine (Baltimore). 2018 Dec;97(52):e13866. doi: 10.1097/MD.0000000000013866.
Mitochondrial encephalopathy, lactic acidosis and stroke-like episodes (MELAS) are thought to be rarely accompanied by macroangiopathy. We reported a case of MELAS that presented right distal internal carotid arterial (ICA) stenosis and reviewed 12 similar previously reported cases involving intracranial large blood vessels.
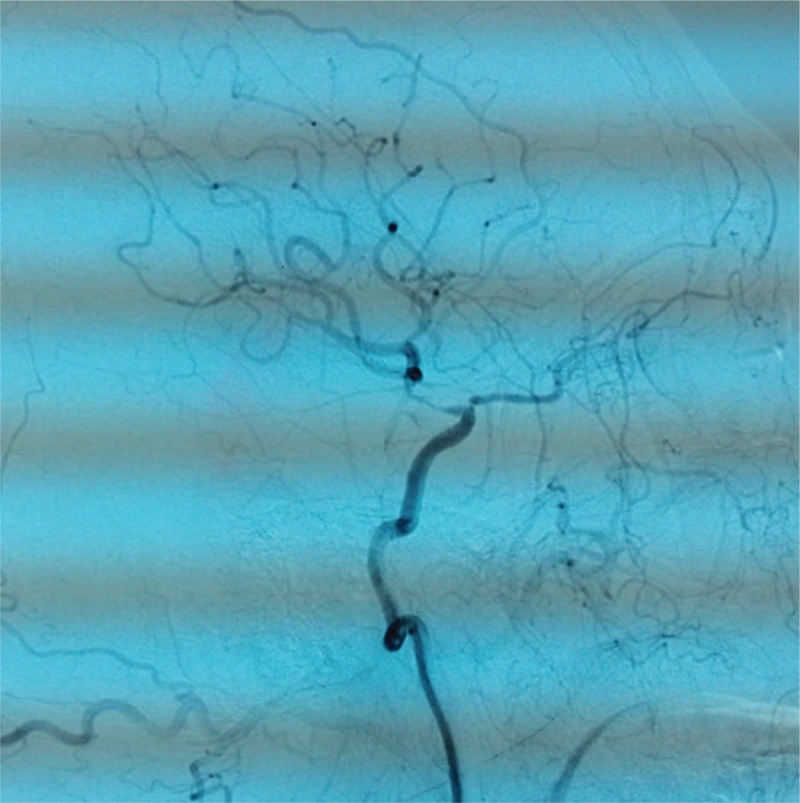
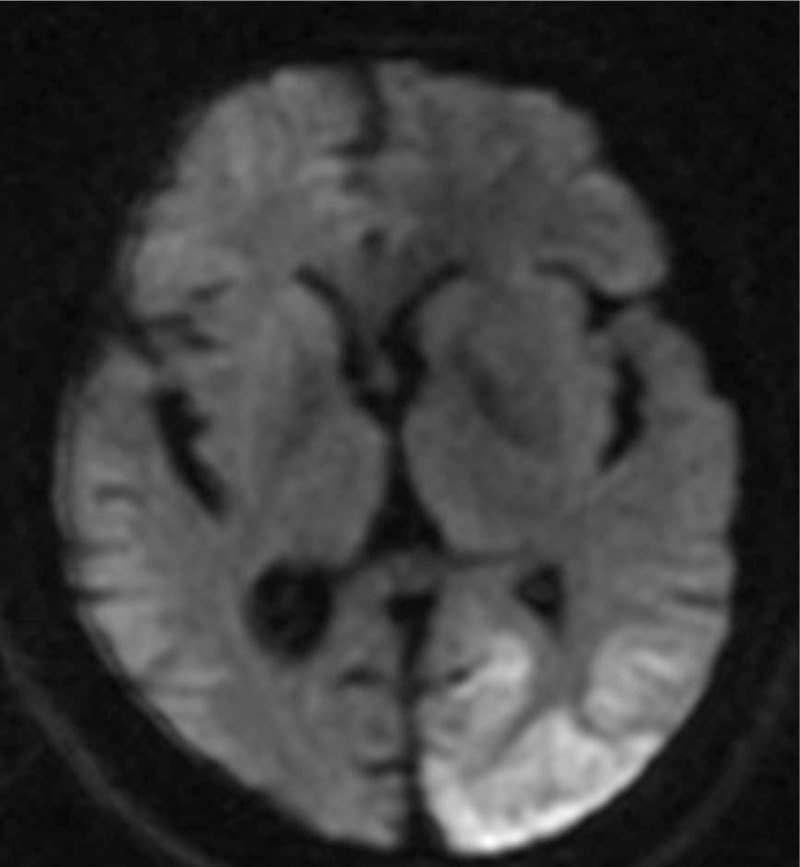
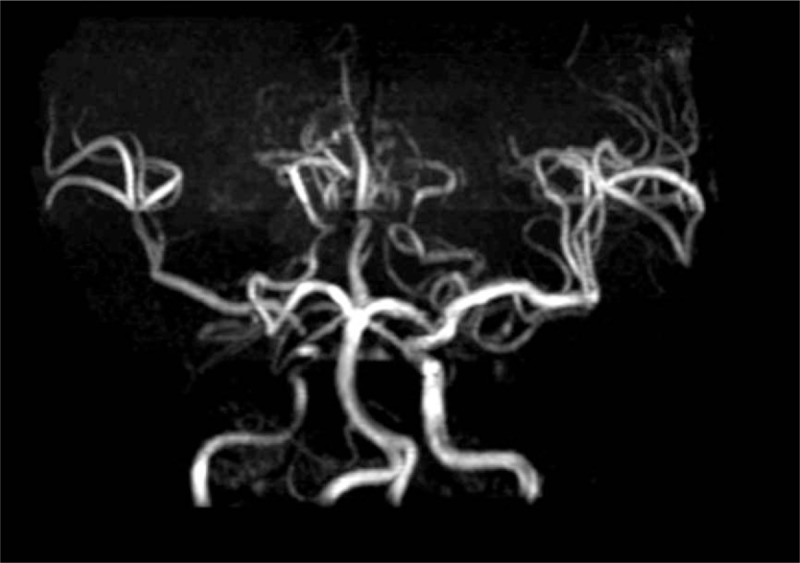
A 38-year-old man suffered from recurrent stroke-like episodes (SE) such as alternating hemiparesis (right lesion 3 years ago and current left lesion), cortical blindness and seizure for 3 years, and was previously misdiagnosed as cerebral infarction. Magnetic Resonance Angiography (MRA) and Digital Subtraction Angiography (DSA) revealed right distal ICA stenosis and sparse cortex blood vessels, which were related to the previous SE.
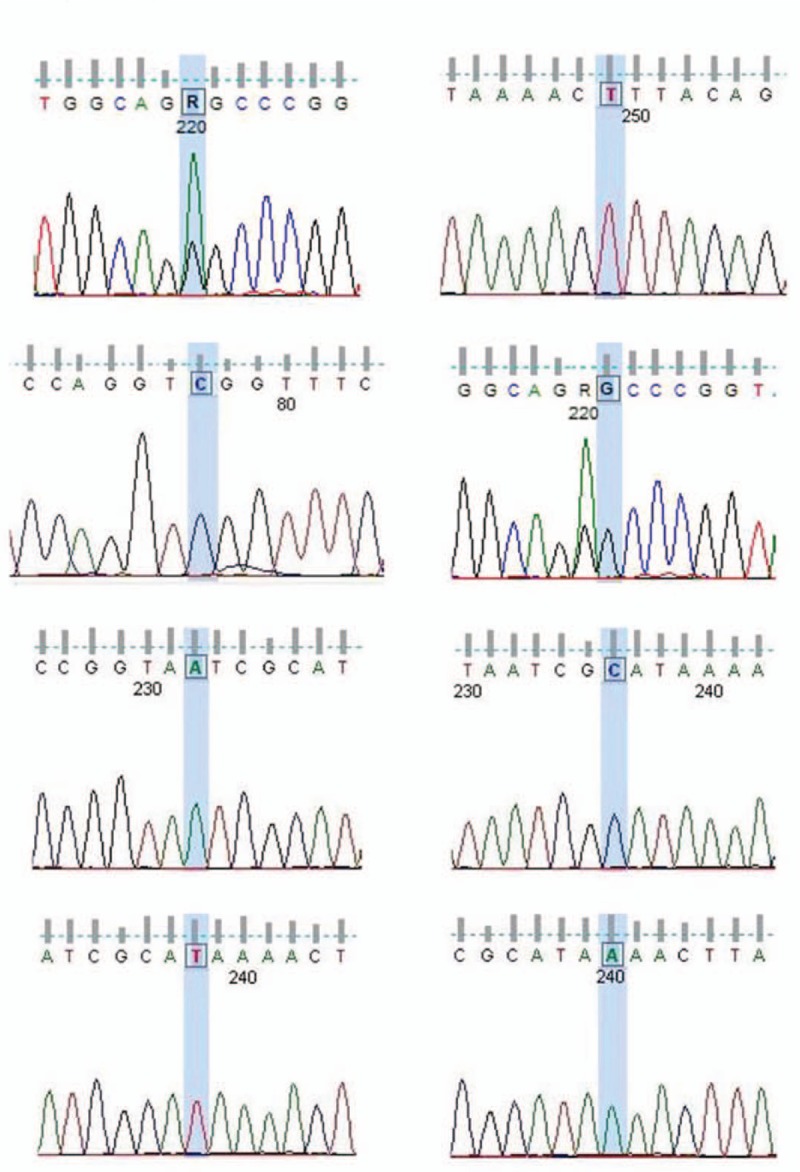
He was diagnosed by genetic screening (a mitochondrial DNA A3243G point mutation) and presence of high lactic acidosis (4.03 mmol/L), which rose to 7.8 mmol/L after exercise.
The patient received Coenzyme Q10, vitamin C, L-arginine for 2 weeks and valproic acid sodium (400 mg bid) to prevent seizures till now.
He is currently less active and intelligent than his peers, with occasional seizures, and needs family care.
Till date, there are 12 reported cases of MELAS combined with major cerebral arteries abnormalities including stenosis, dissection, occlusion, reversible vasoconstriction, aneurysms, and atherosclerosis. Hence, macroangiopathy in MELAS is not very rare. There is correlation between the affected vessels and the lesions in some cases, but not in others, which may increase the misdiagnosis rate. Hence, mitochondrial diseases cannot be excluded due to concurrent macroangiopathic lesions.
线粒体脑肌病伴乳酸血症和卒中样发作(MELAS)被认为很少伴有大血管病变。我们报告了1例出现右侧颈内动脉(ICA)远端狭窄的MELAS病例,并回顾了12例先前报道的涉及颅内大血管的类似病例。
一名38岁男性,3年来反复出现卒中样发作(SE),如交替性偏瘫(3年前右侧病变,目前左侧病变)、皮质盲和癫痫发作,此前被误诊为脑梗死。磁共振血管造影(MRA)和数字减影血管造影(DSA)显示右侧ICA远端狭窄和皮质血管稀疏,这与先前的SE有关。
通过基因筛查(线粒体DNA A3243G点突变)和高乳酸血症(4.03 mmol/L)确诊,运动后升至7.8 mmol/L。
患者接受辅酶Q10、维生素C、L-精氨酸治疗2周,并服用丙戊酸钠(400 mg,每日两次)预防癫痫发作至今。
他目前的活动能力和智力低于同龄人,偶尔发作癫痫,需要家人照顾。
迄今为止,已有12例MELAS合并大脑主要动脉异常的报道,包括狭窄、夹层、闭塞、可逆性血管收缩、动脉瘤和动脉粥样硬化。因此,MELAS中的大血管病变并非十分罕见。在某些病例中,受累血管与病变之间存在相关性,但在其他病例中则不存在,这可能会增加误诊率。因此,不能因并发大血管病变而排除线粒体疾病。