Mohan Bishav, Tandon Rohit, Bansal Raahat, Singh Maninder, Singh Bhupinder, Goyal Abhishek, Chhabra Shibba Takkar, Aslam Naved, Wander Gurpreet S
Department of Cardiology Dayanand Medical College & Hospital Unit Hero, DMC Heart Institute, Ludhiana 141001, Punjab, India.
Department of Cardiology Dayanand Medical College & Hospital Unit Hero, DMC Heart Institute, Ludhiana 141001, Punjab, India.
Indian Heart J. 2018 Dec;70 Suppl 3(Suppl 3):S90-S95. doi: 10.1016/j.ihj.2018.06.008. Epub 2018 Jun 22.
There is limited data regarding in hospital determinants of clinical deterioration and outcome in sub massive pulmonary embolism (PE). We aimed to evaluate these determinants by comparing biomarkers, CT pulmonary angiogram echocardiography, electrocardiography variables.
57 patients of sub massive PE diagnosed on CT pulmonary angiogram were included. All patients received UFH on admission and were divided into two groups based on their clinical course. Group 1 comprised of patients who remained stable, group 2 of patients who showed signs of clinical deterioration.
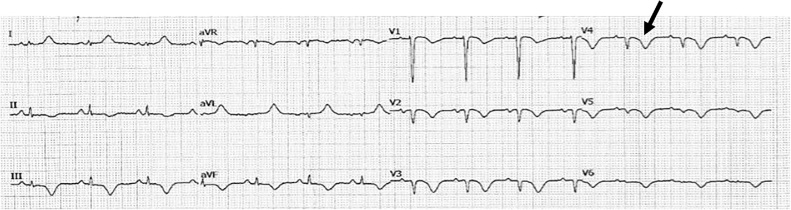
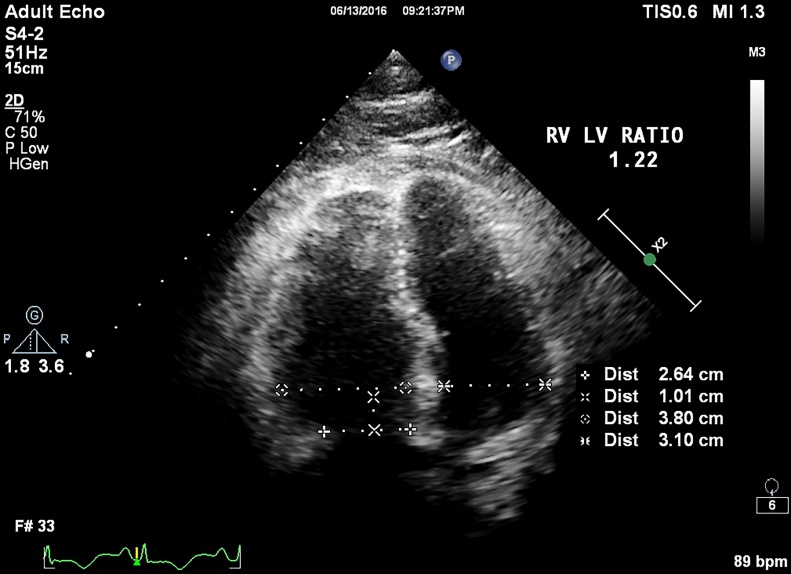
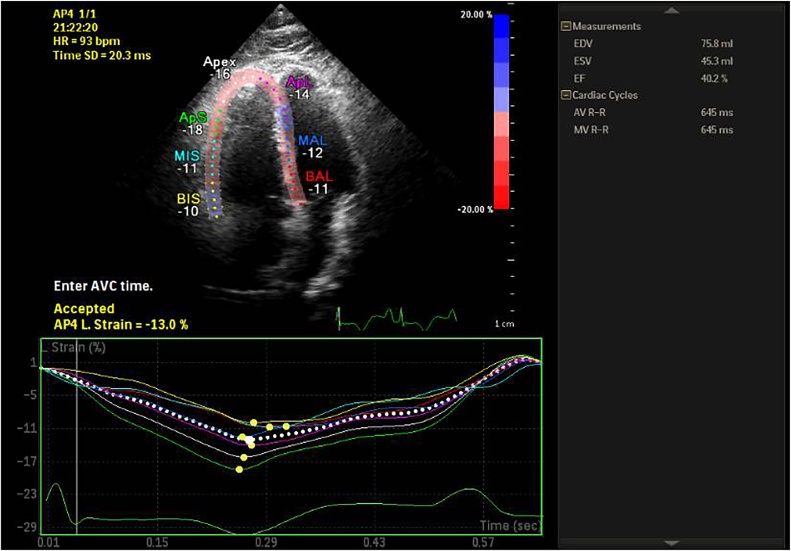
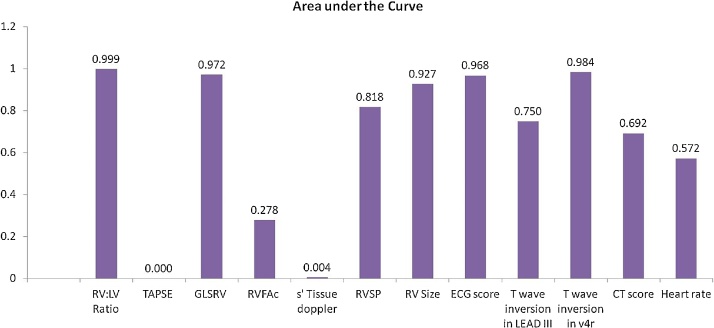
There were 34(59.6%) patients in group 1 and 23(40.4%) patients in group 2. No significant difference in age, gender, BMI. 59.37% had sub massive PE, 5.26% had mortality and 40.4% had clinical deterioration. Intravenous UFH infusion given to 59.6%, systemic thrombolysis 22.8%, catheter directed mechanical breakdown 14%, surgical embolectomy in 3.5% patients. S1Q3T3, new onset RBBB, T wave inversion > 1.63 mm, Basal RV size > 40 mm, RV: LV ratio > 1.2, Global RV longitudinal strain <-10.75% and RVSP > 39 mmHg profiled high risk group. Serum BNP and CT pulmonary angiogram derived scores didn't differ significantly although CT findings helped to exclude low risk patients (specificity 88%, sensitivity 95%).
Physicians should be aware that patients who have ECG and Echocardiography changes suggestive of right ventricular strain and dysfunction above the cut off values and have documented thrombus in Proximal branches (RPA/LPA) or in distal portion of main pulmonary artery may require aggressive management with systemic/catheter based thrombolysis besides routine anticoagulation with heparin to prevent clinical deterioration.
关于亚大面积肺栓塞(PE)患者临床恶化及预后的院内决定因素的数据有限。我们旨在通过比较生物标志物、CT肺动脉造影、超声心动图及心电图变量来评估这些决定因素。
纳入57例经CT肺动脉造影诊断为亚大面积PE的患者。所有患者入院时均接受普通肝素治疗,并根据临床病程分为两组。第1组为病情稳定的患者,第2组为出现临床恶化迹象的患者。
第1组有34例(59.6%)患者,第2组有23例(40.4%)患者。年龄、性别、体重指数无显著差异。59.37%为亚大面积PE,5.26%死亡,40.4%出现临床恶化。59.6%的患者接受静脉普通肝素输注,22.8%接受全身溶栓,14%接受导管定向机械碎栓,3.5%接受手术取栓。S1Q3T3、新发右束支传导阻滞、T波倒置>1.63mm、基底段右心室大小>40mm、右心室与左心室比值>1.2、整体右心室纵向应变<-10.75%及右心室收缩压>39mmHg为高危组特征。血清脑钠肽和CT肺动脉造影得出的评分无显著差异,尽管CT结果有助于排除低风险患者(特异性88%,敏感性95%)。
医生应意识到,心电图和超声心动图显示右心室应变和功能障碍超过临界值且在近端分支(右肺动脉/左肺动脉)或主肺动脉远端有血栓形成记录的患者,除了常规肝素抗凝外,可能还需要积极采用全身或基于导管的溶栓治疗,以防止临床恶化。