Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No. 17, Panjiayuan Nanli, Chaoyang District, Beijing, 100021, P. R. China.
State Key Laboratory of Molecular Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, P. R. China.
Cancer Commun (Lond). 2019 Jan 3;39(1):1. doi: 10.1186/s40880-018-0346-4.
Epithelial-mesenchymal transition (EMT) is implicated in the metastatic process and presents a challenge to epithelial cell adhesion molecule-based detection of circulating tumor cells (CTCs), which have been demonstrated to be a prognostic indicator in metastatic breast cancer. Although evidence has indicated that heterogeneity of CTCs based on EMT markers is associated with disease progression, no standard recommendations have been established for clinical practice. This study aimed to evaluate the prognostic significance of dynamic CTC detection based on EMT for metastatic breast cancer patients.
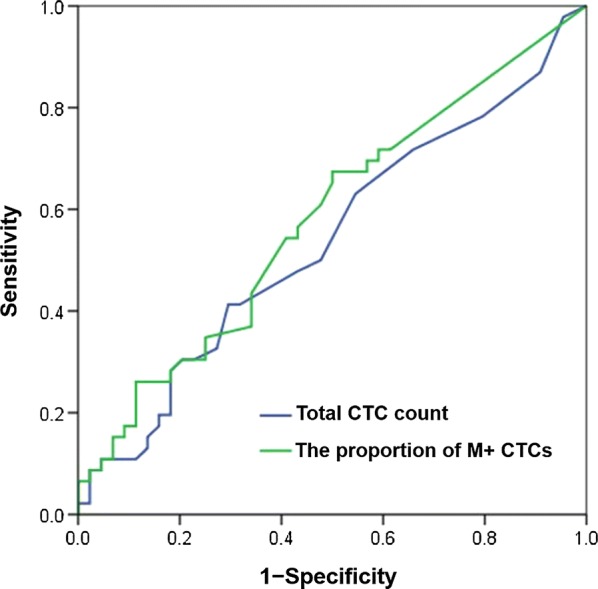
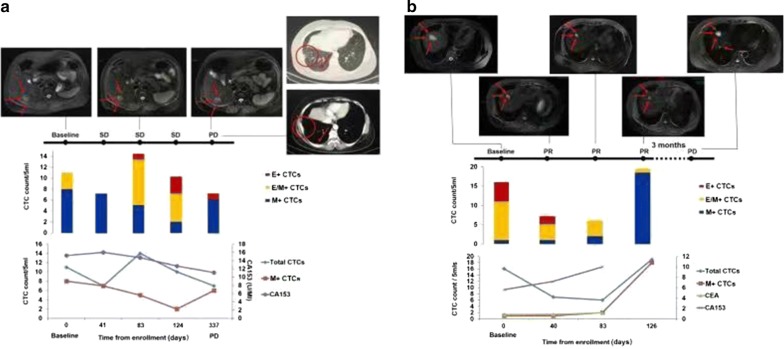
We enrolled 108 human epidermal growth factor receptor 2-negative metastatic breast cancer patients from the prospective phase III CAMELLIA study and applied the CanPatrol CTC enrichment technique to identify CTC phenotypes (including epithelial CTCs, biphenotypic epithelial/mesenchymal CTCs, and mesenchymal CTCs) in peripheral blood samples. Receiver operating characteristic curve analyses of total CTC count and the proportion of mesenchymal CTCs for predicting the 1-year progression-free survival (PFS) rate were conducted to determine the optimal cut-off values, and Kaplan-Meier analysis and Cox proportional hazards regression analysis were performed to investigate the prognostic value of the cut-off values of both total CTC count and the proportion of mesenchymal CTCs in combination.
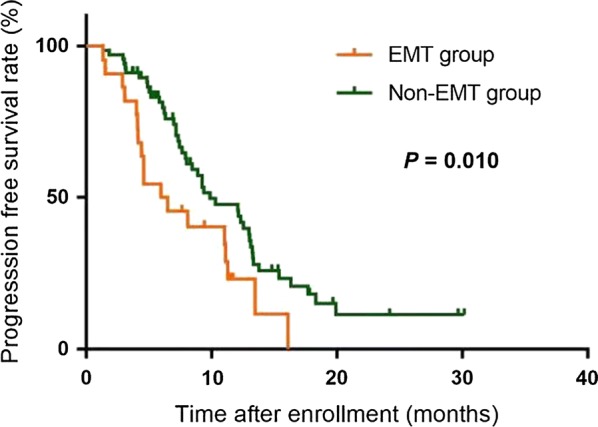
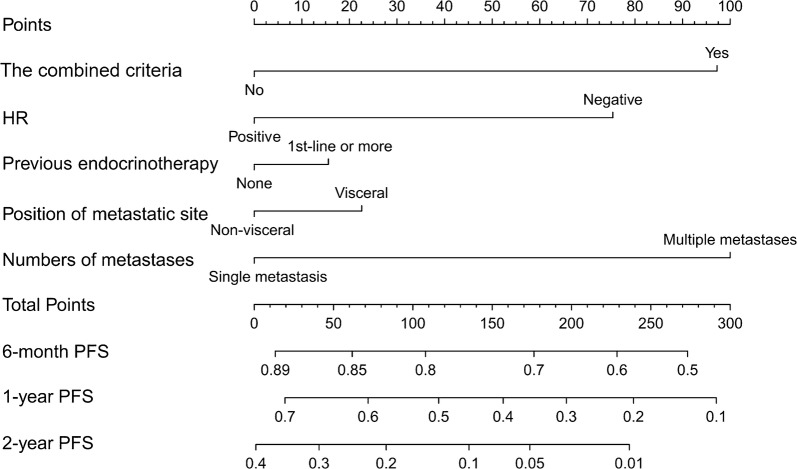
For predicting the 1-year PFS rate, the optimal cut-off value of total CTC count was 9.5 (Area under the curve [AUC] = 0.538, 95% confidence interval [CI] = 0.418-0.657), and that of the proportion of mesenchymal CTCs was 10.7% (AUC = 0.581, 95% CI = 0.463-0.699). We used the two cut-off values in combination to forecast PFS in which the total CTC count was equaled to or exceeded 10/5 mL with the proportion of mesenchymal CTCs surpassed 10.7%. Patients who met the combined criteria had significantly shorter median PFS than did those who did not meet the criteria (6.2 vs. 9.9 months, P =0.010). A nomogram was constructed based on the criteria and significant clinicopathological characteristics with a C-index of 0.613 (P = 0.010).
The criteria, which combine the total CTC count and the proportion of mesenchymal CTCs, may be used to monitor therapeutic resistance and predict prognosis in patients with metastatic breast cancer. Trial registration ClinicalTrials.gov. NCT01917279. Registered on 19 July 2013, https://clinicaltrials.gov/ct2/show/NCT01917279?term=NCT01917279&rank=1 .
上皮-间充质转化(EMT)与转移过程有关,并对基于上皮细胞黏附分子的循环肿瘤细胞(CTC)检测提出了挑战,后者已被证明是转移性乳腺癌的预后指标。尽管有证据表明,基于 EMT 标志物的 CTC 异质性与疾病进展相关,但尚未为临床实践制定标准建议。本研究旨在评估基于 EMT 的动态 CTC 检测对转移性乳腺癌患者的预后意义。
我们从前瞻性 III 期 CAMELLIA 研究中招募了 108 名人表皮生长因子受体 2 阴性转移性乳腺癌患者,并应用 CanPatrol CTC 富集技术在外周血样本中鉴定 CTC 表型(包括上皮 CTC、双表型上皮/间充质 CTC 和间充质 CTC)。进行总 CTC 计数和间充质 CTC 比例的受试者工作特征曲线分析,以确定预测 1 年无进展生存期(PFS)率的最佳截断值,并进行 Kaplan-Meier 分析和 Cox 比例风险回归分析,以研究总 CTC 计数和间充质 CTC 比例截断值组合的预后价值。
对于预测 1 年 PFS 率,总 CTC 计数的最佳截断值为 9.5(曲线下面积[AUC] = 0.538,95%置信区间[CI] = 0.418-0.657),间充质 CTC 比例的截断值为 10.7%(AUC = 0.581,95%CI = 0.463-0.699)。我们使用这两个截断值的组合来预测 PFS,其中总 CTC 计数等于或超过 10/5 mL,间充质 CTC 比例超过 10.7%。符合联合标准的患者的中位 PFS明显短于不符合标准的患者(6.2 与 9.9 个月,P =0.010)。基于标准和具有统计学意义的临床病理特征构建了一个列线图,C 指数为 0.613(P = 0.010)。
这些标准将总 CTC 计数和间充质 CTC 比例相结合,可用于监测治疗耐药性并预测转移性乳腺癌患者的预后。试验注册ClinicalTrials.gov。NCT01917279。于 2013 年 7 月 19 日注册,https://clinicaltrials.gov/ct2/show/NCT01917279?term=NCT01917279&rank=1。