Department of Epidemiology and Preventive Medicine, School of Public Health and Preventive Medicine, Monash University, Melbourne, Australia.
International Centre for Diarrheal Disease Research, Bangladesh (icddr,b), Dhaka, Bangladesh.
Am J Trop Med Hyg. 2019 Mar;100(3):742-749. doi: 10.4269/ajtmh.18-0644.
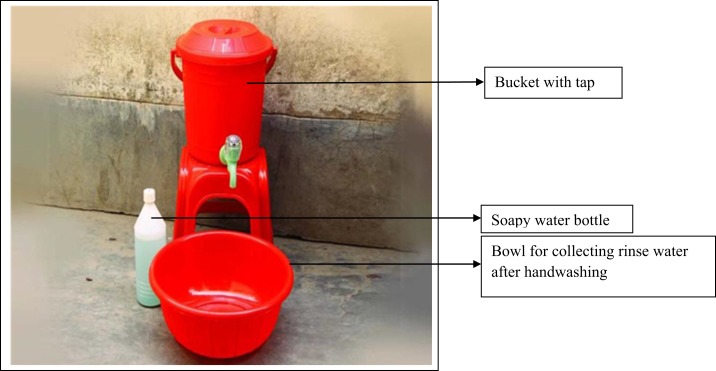
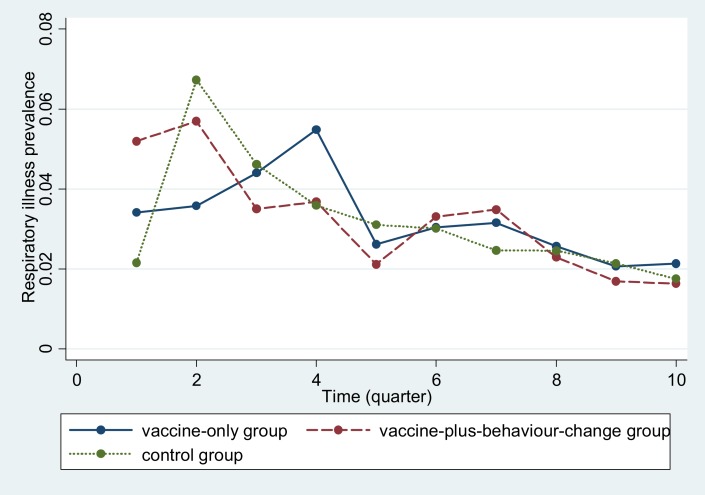
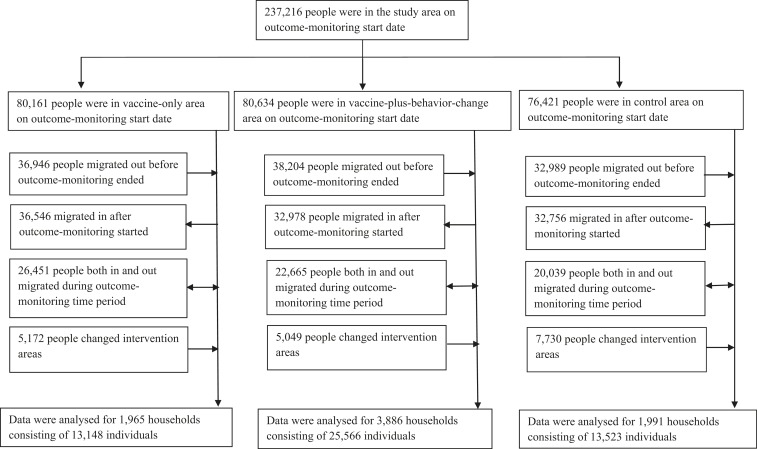
We assessed the impact of handwashing promotion on reported respiratory illness as a secondary outcome from among > 60,000 low-income households enrolled in a cluster-randomized trial conducted in Bangladesh. Ninety geographic clusters were randomly allocated into three groups: cholera-vaccine-only; vaccine-plus-behavior-change (handwashing promotion and drinking water chlorination); and control. Data on respiratory illness (fever plus either cough or nasal congestion or breathing difficulty within previous 2 days) and intervention uptake (presence of soap and water at handwashing station) were collected through monthly surveys conducted among a different subset of randomly selected households during the intervention period. We determined respiratory illness prevalence across groups and used log-binomial regression to examine the association between respiratory illness and presence of soap and water in the handwashing station. Results were adjusted for age, gender, wealth, and cluster-randomized design. The vaccine-plus-behavior-change group had more handwashing stations with soap and water present than controls (45% versus 25%; < 0.001). Reported respiratory illness prevalence was similar across groups (vaccine-plus-behavior-change versus control: 2.8% versus 2.9%; 95% confidence interval [CI]: -0.008, 0.006; = 0.6; cholera-vaccine-only versus control: 3.0% versus 2.9%; 95% CI: -0.006, 0.009; = 0.4). Irrespective of intervention assignment, respiratory illness was lower among people who had soap and water present in the handwashing station than among those who did not (risk ratio: 0.82; 95% CI: 0.69-0.98). With modest uptake of the handwashing intervention, we found no impact of this large-scale intervention on respiratory illness. However, those who actually had a handwashing station with soap and water had less illness. This suggests improving the effectiveness of handwashing promotion in achieving sustained behavior change could result in health benefits.
我们评估了手卫生促进对孟加拉国开展的一项随机对照试验中超过 6 万户低收入家庭报告的呼吸道疾病的影响。90 个地理区域被随机分为三组:霍乱疫苗组;疫苗加行为改变组(手卫生促进和饮用水氯化消毒);对照组。在干预期间,通过对不同随机选择的家庭进行每月调查,收集呼吸道疾病(发热伴有咳嗽或鼻塞或呼吸困难)和干预措施采用情况(洗手站是否有肥皂和水)的数据。我们比较了各组的呼吸道疾病流行率,并使用对数二项回归分析了在洗手站有肥皂和水与呼吸道疾病之间的关联。结果根据年龄、性别、财富和集群随机设计进行了调整。行为改变加疫苗组拥有更多配有肥皂和水的洗手站(45%比 25%;<0.001)。各组报告的呼吸道疾病流行率相似(行为改变加疫苗组与对照组:2.8%比 2.9%;95%置信区间[CI]:-0.008,0.006;=0.6;霍乱疫苗组与对照组:3.0%比 2.9%;95% CI:-0.006,0.009;=0.4)。无论干预措施如何,在洗手站有肥皂和水的人患呼吸道疾病的风险低于没有肥皂和水的人(风险比:0.82;95% CI:0.69-0.98)。尽管手卫生干预措施的采用率不高,但我们发现这种大规模干预措施对呼吸道疾病没有影响。然而,那些确实有带肥皂和水的洗手站的人患病的情况较少。这表明,提高手卫生促进的有效性以实现持续的行为改变可能会带来健康益处。