1 University department of Cardiac Surgery Leipzig Heart Center Germany.
J Am Heart Assoc. 2019 Jan 8;8(1):e010940. doi: 10.1161/JAHA.118.010940.
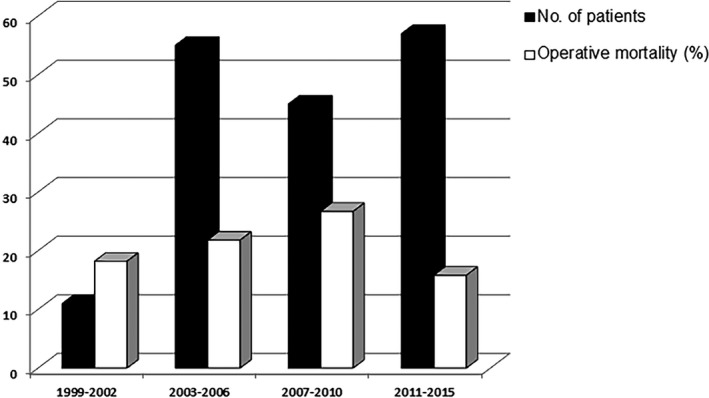
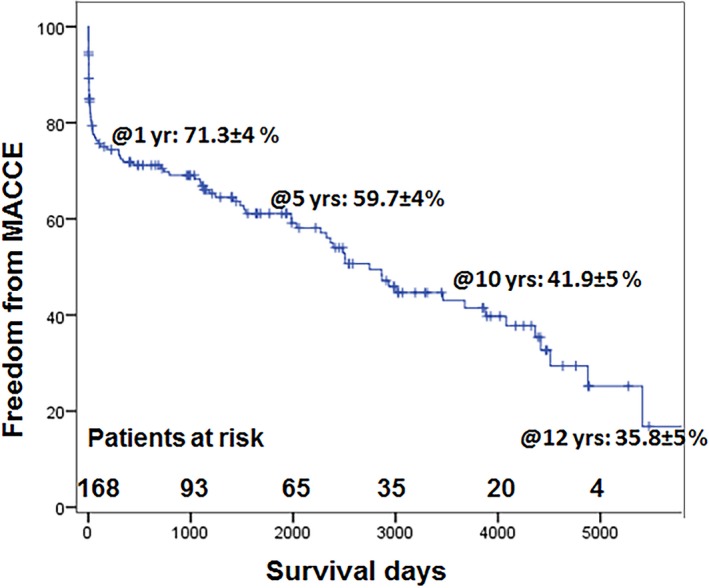
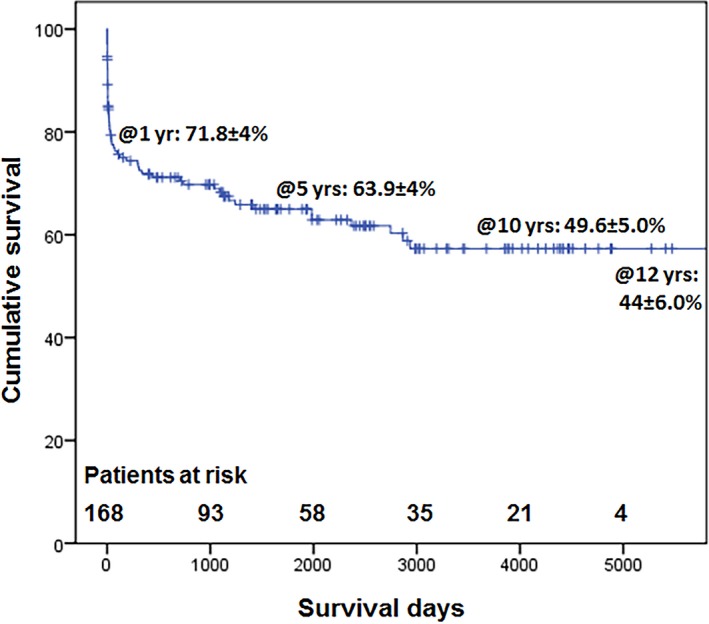
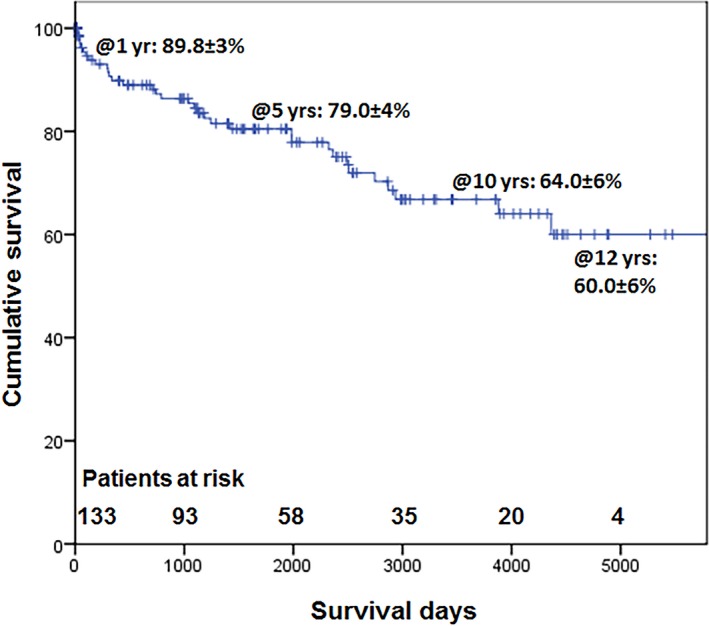
Background Iatrogenic coronary artery injuries during percutaneous coronary interventions ( PCI ) often require emergent surgical management. Our study evaluated the early and long-term outcomes in patients undergoing surgical treatment of iatrogenic PCI complications and identified the predictors of operative and long-term mortality. Methods and Results Pre-, intra- and post-operative data and hospital outcomes of 168 consecutive patients undergoing cardiac surgical procedures for iatrogenic complications following PCI between December 1999 and July 2015, were prospectively collected in our computerized database. Logistic and Cox regression analyses were used to identify the independent predictors of operative and long-term mortality. The mean age was 68.5±10.2 years and 35.7% were females. PCI complications included left anterior descending (38.7%), right coronary (29.2%), circumflex (13.1%), left main coronary artery injuries (19.0%), and acute myocardial infarction (66.7%), Type A aortic dissection (7.7%), cardiac tamponade (17.9%), and cardiogenic shock ( CS ) (46.4%). Operative mortality for corrective surgery was 20.8% and was independently predicted by critical preoperative state (odds ratio: 3.5; P=0.01). The 5- and 10-year survival for all patients was 63.9±4.0% and 49.6±5.0%, which improved remarkably in hospital survivors (79.0±4.0% and 64.0±6.0%). Risk factors for long-term mortality were critical preoperative state (hazard ratio: 3.5; P<0.0001) and coronary artery occlusion during PCI (hazard ratio: 2.6; P=0.002). The 5- and 10-year freedom from major adverse cardiac and cerebrovascular events was 59.7±4.0% and 41.9±5.0%. Conclusions Iatrogenic injuries after PCI or coronary angiography requiring surgical correction are associated with a high operative and long-term mortality. Patients developing acute coronary artery occlusion have a more guarded long-term prognosis. Hospital survivors, however, have a superior long-term survival.
经皮冠状动脉介入治疗(PCI)过程中发生的医源性冠状动脉损伤常需要紧急外科治疗。我们的研究评估了因 PCI 并发症而行外科治疗的患者的早期和长期结局,并确定了手术和长期死亡率的预测因素。
1999 年 12 月至 2015 年 7 月,前瞻性地在我们的计算机数据库中收集了 168 例连续患者接受心脏手术治疗医源性 PCI 并发症的术前、术中及术后数据和住院结局。使用逻辑回归和 Cox 回归分析确定手术和长期死亡率的独立预测因素。患者平均年龄为 68.5±10.2 岁,35.7%为女性。PCI 并发症包括左前降支(38.7%)、右冠状动脉(29.2%)、回旋支(13.1%)、左主干冠状动脉损伤(19.0%)、急性心肌梗死(66.7%)、A型主动脉夹层(7.7%)、心脏压塞(17.9%)和心源性休克(CS)(46.4%)。择期手术死亡率为 20.8%,术前危急状态是独立预测因素(优势比:3.5;P=0.01)。所有患者的 5 年和 10 年生存率分别为 63.9±4.0%和 49.6±5.0%,住院幸存者的生存率显著提高(79.0±4.0%和 64.0±6.0%)。长期死亡率的危险因素是术前危急状态(危险比:3.5;P<0.0001)和 PCI 期间冠状动脉闭塞(危险比:2.6;P=0.002)。5 年和 10 年免于主要不良心脑血管事件的发生率分别为 59.7±4.0%和 41.9±5.0%。
需要外科矫正的 PCI 或冠状动脉造影后的医源性损伤与较高的手术和长期死亡率相关。发生急性冠状动脉闭塞的患者有更差的长期预后。然而,住院幸存者具有更好的长期生存率。