Division of Transfusion Medicine, Department of Pathology, Johns Hopkins University, Baltimore, Maryland.
Transfusion. 2019 Apr;59(4):1291-1299. doi: 10.1111/trf.15139. Epub 2019 Jan 8.
Bacterial contamination of platelets remains the leading infectious risk from blood transfusion. Pathogen reduction (PR), point-of-release testing (PORt), and secondary bacterial culture (SBC) have been proposed as alternative risk control strategies, but a comprehensive financial comparison has not been conducted.
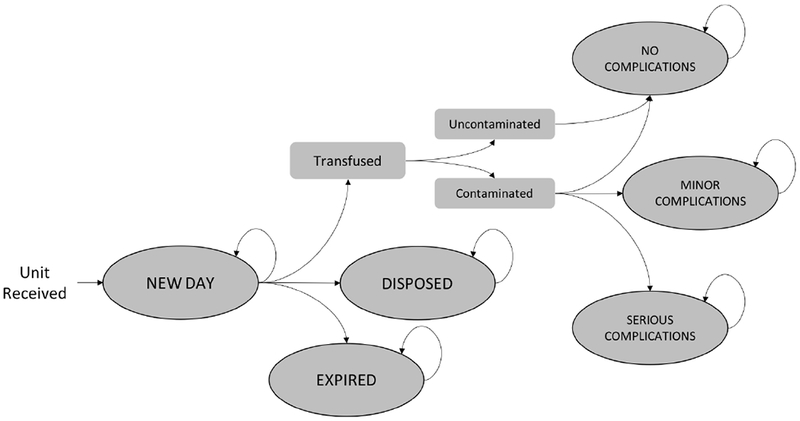
A Markov-based decision tree was constructed to model the financial and clinical impact of PR, PORt, and SBC, as well as a baseline strategy involving routine testing only. Hospitals were assumed to acquire leukoreduced apheresis platelets on Day 3 after collection, and, in the base case analysis, expiration would occur at the end of Day 5 (PR and SBC) or 7 (PORt). Monte Carlo simulations assessed the direct medical costs for platelet acquisition, testing, transfusion, and possible complications. Input parameters, including test sensitivity and specificity, were drawn from existing literature, and costs (2018 US dollars) were based on a hospital perspective.
The total costs per unit acquired by the hospital under the baseline strategy, PR, PORt, and SBC were $651.45, $827.82, $686.33, and $668.50, respectively. All risk-reduction strategies decreased septic transfusion reactions and associated expenses, with the greatest reductions from PR. PR would add $191.09 in per-unit acquisition costs, whereas PORt and SBC would increase per-unit testing costs by $31.79 and $17.26, respectively. Financial outcomes were sensitive to platelet dating; allowing 7-day storage with SBC would lead to a cost savings of $12.41 per transfused unit. Results remained robust in probabilistic sensitivity analyses.
All three strategies are viable approaches to reducing bacterially contaminated platelet transfusions, although SBC is likely to be the cheapest overall.
血小板的细菌污染仍然是输血相关感染的主要风险。病原体减少(PR)、放行检测(PORt)和二次细菌培养(SBC)已被提议作为替代风险控制策略,但尚未进行全面的财务比较。
构建了一个基于马尔可夫的决策树模型,用于模拟 PR、PORt 和 SBC 以及仅常规检测的基线策略的财务和临床影响。假设医院在采集后的第 3 天获取去白细胞的单采血小板,在基本案例分析中,血小板的有效期将在第 5 天(PR 和 SBC)或第 7 天(PORt)结束。蒙特卡罗模拟评估了血小板获取、检测、输血和可能并发症的直接医疗成本。输入参数包括测试的灵敏度和特异性,这些参数均取自现有文献,而成本(2018 年美元)则基于医院视角。
在基线策略、PR、PORt 和 SBC 下,医院每单位获得的总成本分别为 651.45 美元、827.82 美元、686.33 美元和 668.50 美元。所有降低风险的策略都降低了败血症输血反应和相关费用,其中 PR 的降低幅度最大。PR 将使每单位的获得成本增加 191.09 美元,而 PORt 和 SBC 将使每单位的检测成本分别增加 31.79 美元和 17.26 美元。财务结果对血小板日期敏感;允许 SBC 储存 7 天,每输注单位将节省 12.41 美元。概率敏感性分析结果仍然稳健。
三种策略都是减少细菌污染血小板输血的可行方法,尽管 SBC 总体上可能是最便宜的。